
What is spinal stenosis?
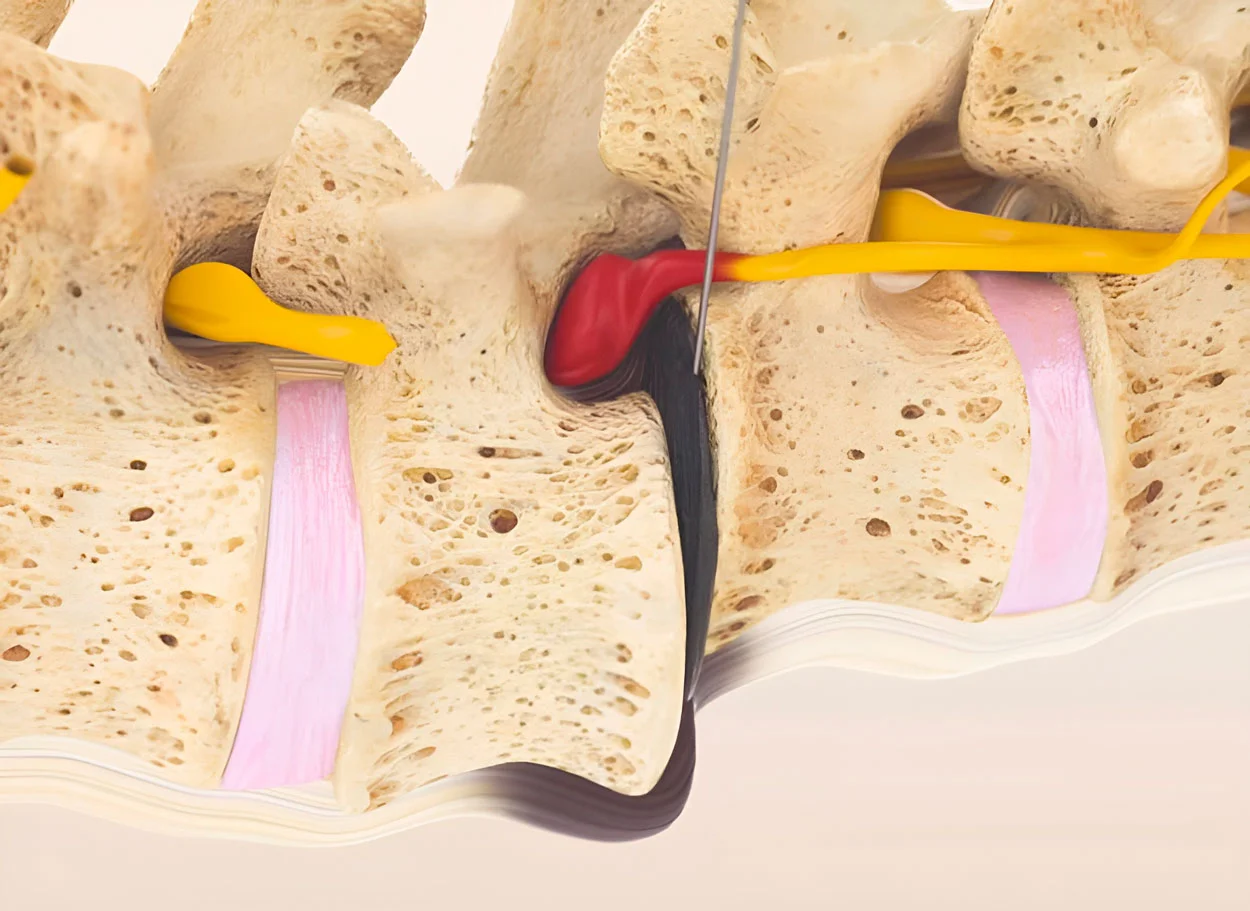
Spinal stenosis is a pathological narrowing of the spinal canal lumen through which the spinal cord and nerve roots pass. The narrowing leads to compression of neural structures and impaired blood supply, causing pain, numbness, and weakness in the extremities.
This is one of the most common spine diseases in people over 50 years old. According to research data, stenosis is detected in 20-30% of people over 60 years old on MRI, although it is not clinically manifest in all cases.
Types of stenosis:
- Central stenosis — narrowing of the central canal, compression of the spinal cord
- Lateral (foraminal) stenosis — narrowing of the intervertebral foramen, compression of the nerve root
- Degenerative stenosis — the most common, develops with age
- Congenital stenosis — anatomically narrow spinal canal
Causes of development:
- Hypertrophy of the ligamentum flavum
- Osteophytes (bone spurs)
- Disc herniations and protrusions
- Spondylolisthesis
- Facet joint osteoarthritis
Facts about stenosis
- ICD-10: M48.0
- Incidence: 5 per 100,000 people per year
- Age: most common over 50 years
- Location: 75% — lumbar spine
- Surgeries: the most common reason for spine surgery in the elderly
Causes and mechanism of development
Spinal stenosis is the result of degenerative changes that accumulate over years. With age, spine structures thicken and deform, gradually narrowing the canal lumen through which the spinal cord and nerve roots pass.
Degenerative causes
- Hypertrophy of the ligamentum flavum — thickening of the ligament that limits the canal posteriorly. The main cause of stenosis
- Osteophytes — bony growths on vertebral bodies and facet joints
- Facet Joint Osteoarthritis — joint enlargement narrows the lateral recesses
- Herniations and Disc Protrusions — disc bulging into the canal lumen
- Spondylolisthesis — vertebral displacement deforming the canal
Other Causes
- Congenital Stenosis — anatomically narrow canal from birth (diameter less than 12 mm)
- Post-Traumatic — after vertebral fractures
- Iatrogenic — after previous surgeries (scarring, instability)
- Paget's Disease — bone thickening
- Ligament Calcification — calcium salt deposition
Why MIBRAR® is Effective for Stenosis
- Regenerative concentrates reduce hypertrophy of the ligamentum flavum
- Anti-inflammatory effect reduces tissue swelling in the stenosis area
- Stem cells initiate remodeling — "restructuring" of tissues
- No need for bone removal (laminectomy) or fixation (spinal fusion)
- Spinal mobility is fully preserved
Symptoms of Spinal Stenosis
Lumbar Stenosis
- Neurogenic (spinal) claudication
- Pain and heaviness in legs when walking
- Relief when bending forward
- Numbness and tingling in legs
- Weakness in legs
- Reduced walking distance
Cervical Stenosis
- Pain and stiffness in the neck
- Numbness in arms
- Impaired fine motor skills
- Impaired coordination when walking
- In severe cases — myelopathy
⚠️ Red Flags
- Bladder dysfunction
- Progressive weakness in legs
- Gait disturbance
- Cauda equina syndrome
Diagnosis of Stenosis
Accurate diagnosis of stenosis is critically important, as symptoms may mimic vascular leg diseases (intermittent claudication). The key differential feature: with stenosis, pain decreases when bending forward (canal expands), while with vascular pathology — when stopping.
Diagnostic Methods:
- MRI — primary method. Visualizes the degree of canal narrowing, ligament hypertrophy, disc and nerve root condition. Measures the cross-sectional area of the canal (normal — more than 100 mm², severe stenosis — less than 75 mm²)
- CT — details bony changes: osteophytes, calcifications, vertebral arch deformities
- Functional X-rays — detect instability and spondylolisthesis during flexion/extension
- EMG — assesses the degree of nerve damage and helps differentiate stenosis from polyneuropathy
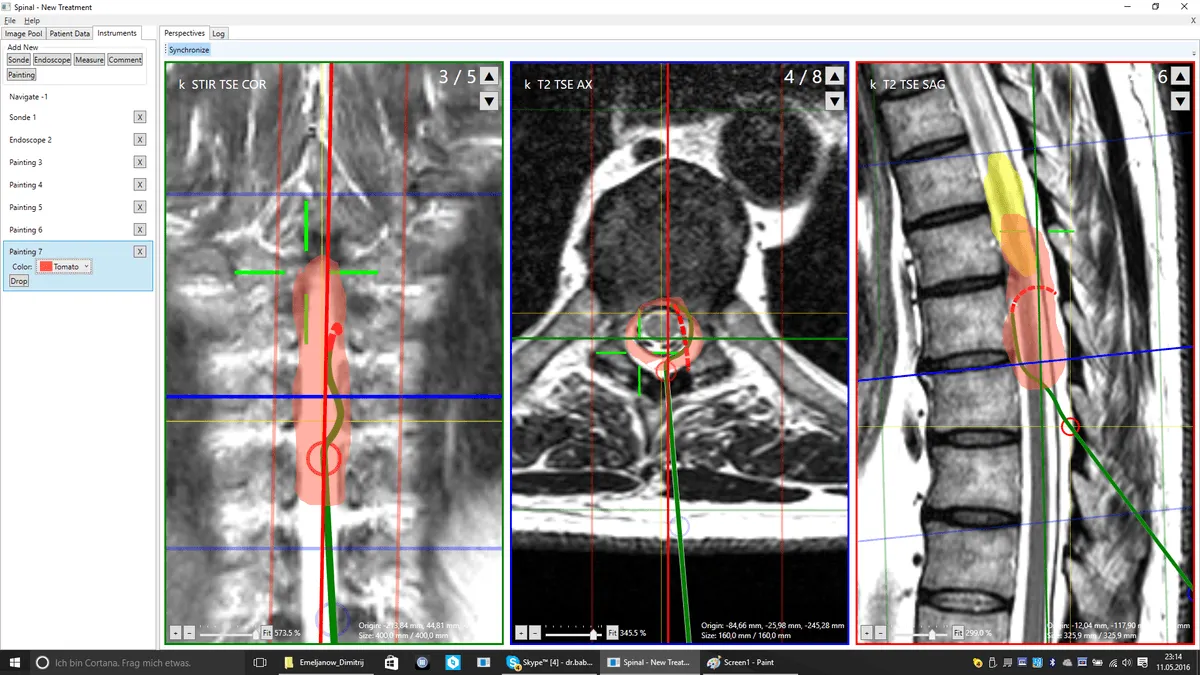
MIBRAR® Treatment Planning:
MRI/CT images are uploaded to the Cyber Navi Hand™ system, which creates a 3D map of compression zones. The surgeon precisely identifies which structures cause narrowing (ligamentum flavum, osteophytes, discs) and plans injection sites for regenerative concentrates for maximum decompression effect.
Free MRI Evaluation
- Send MRI images online
- Prof. Babayan will personally assess the degree of stenosis
- Report within 48 hours
- No obligations
Traditional Stenosis Treatment vs MIBRAR®
| Criterion | Laminectomy / Spinal Fusion | Epidural Blocks | MIBRAR® |
|---|---|---|---|
| Principle | Surgical removal of bone/ligaments | Steroids to reduce inflammation | Tissue regeneration, reduction of compression |
| Anesthesia | General anesthesia | Local anesthesia | No anesthesia |
| Hospitalization | 5-10 days | No | No — home the same day |
| Recovery | 3-6 months | 1-3 days | Several days |
| Risks for elderly | High (general anesthesia, infection) | Low | Minimal — ideal for elderly |
| Mobility preservation | Reduced (with spinal fusion) | No effect | Fully preserved |
How MIBRAR® treats Spinal Stenosis
Precise diagnostics
MRI images are analyzed by the Cyber Navi Hand™ system. Exact zones of compression, degree of canal narrowing, and condition of surrounding tissues are determined. A 3D plan for micro-invasive access is created.
Obtaining concentrates
CGF concentrate with growth factors and stem cells is obtained from the patient's blood. In cases of pronounced Spinal Stenosis, Lipogems® — mesenchymal stem cell concentrate from adipose tissue — is additionally prepared.
Micro-invasive injection
Under navigational control, concentrates are injected into the stenosis zone: into the hypertrophied yellow ligament, facet joint area, around nerve roots. Growth factors initiate tissue remodeling.
Regeneration and remodeling
Stem cells reduce ligament hypertrophy, decrease inflammation and edema in the stenosis zone. This leads to expansion of the effective canal lumen and decompression of neural structures without bone removal.
Why MIBRAR® is effective for Spinal Stenosis
Spinal Stenosis is a condition where traditional surgery is often the only option. Laminectomy (removal of part of the vertebral arch) widens the canal but at the cost of Spine stability. Spondylolisthesis (vertebral fixation) restores stability but completely blocks segmental mobility. MIBRAR® offers a third path — biological tissue remodeling without surgery.
Mechanism of action for Spinal Stenosis:
- Reduction of yellow ligament hypertrophy — growth factors initiate restructuring of collagen fibers, reducing ligament thickness and expanding the effective canal lumen
- Anti-inflammatory effect — CGF and Lipogems® suppress chronic inflammation in the stenosis zone, reducing tissue edema and nerve root compression
- Neuroprotection — growth factors (VEGF, NGF) improve blood supply to neural structures and promote recovery of conductivity in damaged nerves
- Disc regeneration — when stenosis is combined with disc degeneration (in 70-80% of cases), disc height is simultaneously restored, further expanding foraminal openings
Important: MIBRAR® is especially valuable for elderly patients (over 65-70 years) for whom general anesthesia and extensive surgery are contraindicated due to comorbidities. The procedure is performed under local anesthesia, outpatient, without hospitalization.
MIBRAR® for Spinal Stenosis
- No laminectomy — no bone removal
- No Spondylolisthesis — mobility preserved
- No anesthesia — local anesthesia
- No hospitalization — home the same day
- Multiple zones — stenosis + herniations + osteoarthritis simultaneously
- Any age — including patients 70-90 years old
Treatment Results for Spinal Stenosis
Follow-up MRI scans demonstrate spinal canal widening and decompression of neural structures after the MIBRAR® procedure.

MIBRAR Case: Female, 38 years
Diagnosis: Compressive spinal canal stenosis C4-C6, herniations C4/C5 (1.9 mm) and C5/C6 (5.8 mm), osteochondrosis C3-C7, cervical kyphosis. Finger numbness, headaches.
Result: Immediately after surgery — complete pain resolution. Follow-up MRI shows C5/C6 herniation is no longer detectable. Patient actively participates in sports.
View case study →
MIBRAR Case: Female, 43 years
Diagnosis: Post radiofrequency nucleotomy. Complete disc wear at L5/S1, pseudoretrolisthesis L4 and L5, bilateral neuroforaminal stenosis, lumbosacral destabilization.
Result at 18 months: Complete reconstruction of disc height and shape at L4/L5 and L5/S1, elimination of retrolisthesis, restoration of sagittal balance. One week post-surgery — complete symptom resolution.
View case study →MIBRAR® Method Advantages
95% of interventions covered
MIBRAR® covers up to 95% of all spinal neurosurgery and orthopedic operations.
No anesthesia or incisions
Outpatient treatment via 0.3-1.5 mm puncture. No general anesthesia or hospitalization.
No age restrictions
Regeneration at any age. Safe for chronic conditions and anesthesia intolerance.
Rapid improvement
Concentrates have analgesic and anti-inflammatory properties. Relief within days.
Multiple zones at once
Simultaneous treatment of multiple discs or joints in one procedure.
Home the same day
No crutches, braces or rehabilitation needed. MRI follow-up at 8-16 weeks.
MIBRAR® Technology
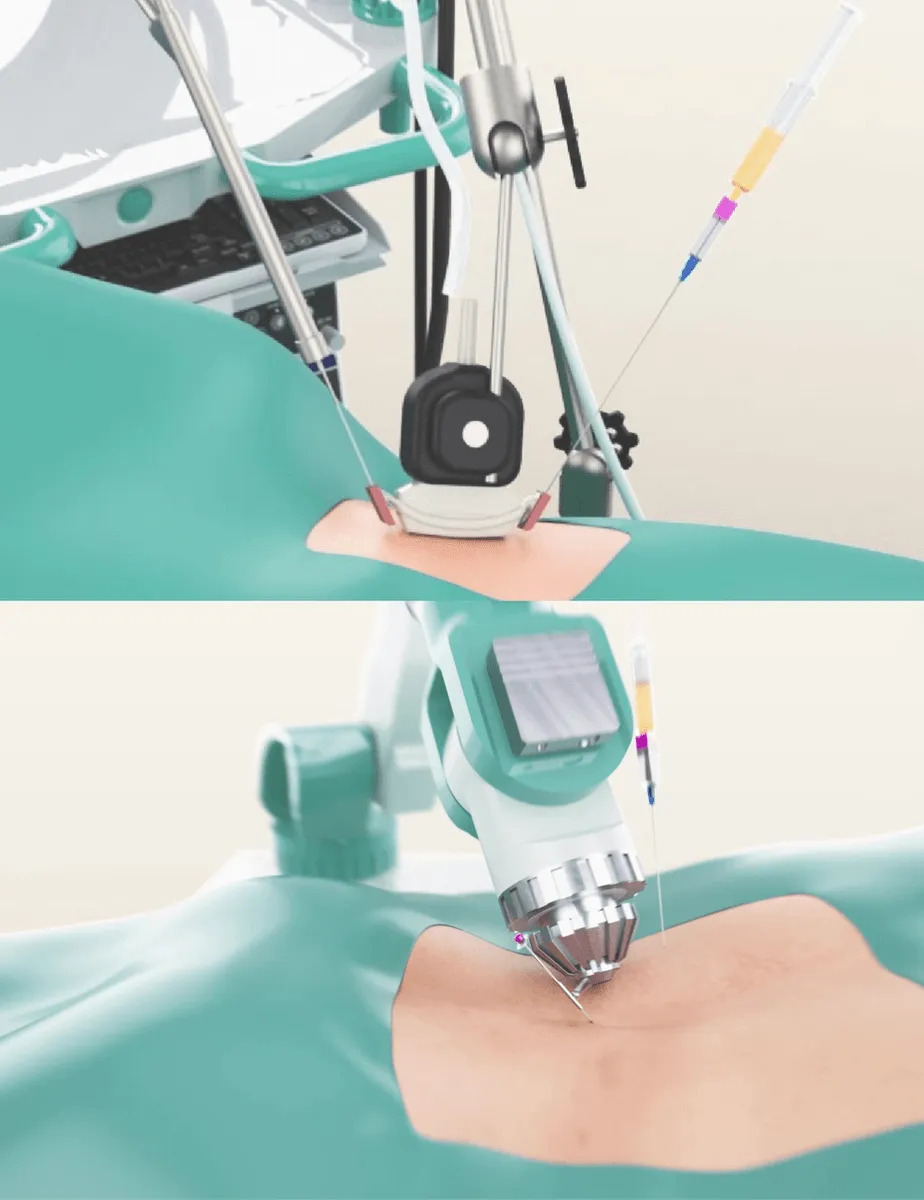
Cyber Navi Hand™
Intraoperative robotic navigation system. Provides precise access to deep structures with 1 mm and 1 degree accuracy.

Sono Control Arm™
Device for intervention under sonographic control. Eliminates open surgeries with real-time visual monitoring.