
Video about the MIBRAR® Method
What is radiculopathy
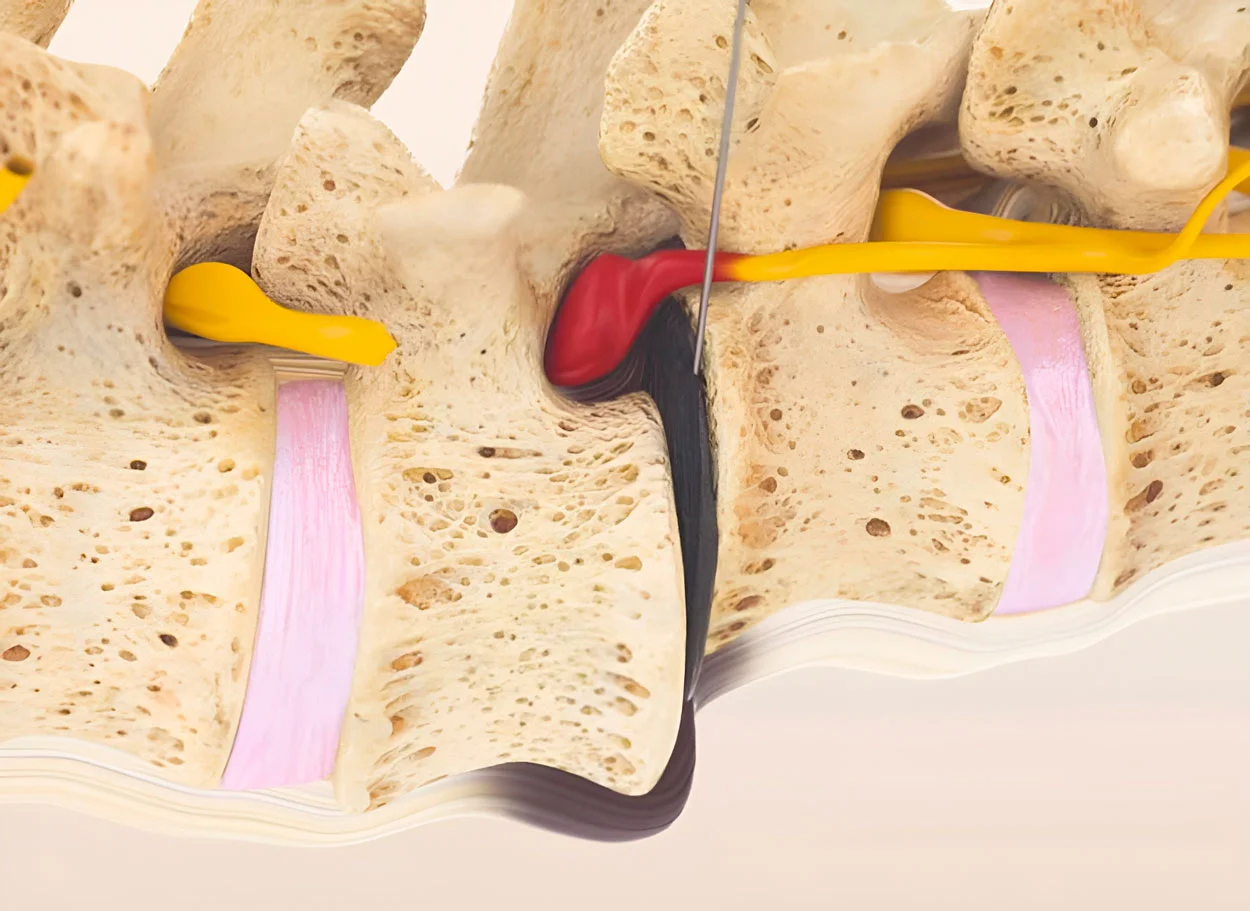
Radiculopathy is damage to a nerve root due to its compression at the level of exit from the spinal canal. In everyday terms, this is called "nerve compression" or "radiculitis." Radiculopathy is not a diagnosis, but a syndrome with a specific underlying cause.
Causes of radiculopathy
Herniated disc/disc protrusion (80%)
Bulging or rupture of the disc compresses the nerve root. The most common cause in patients aged 30-50 years. L4-L5 and L5-S1 — 95% of lumbar radiculopathies. C5-C6 and C6-C7 — 90% of cervical.
Foraminal stenosis (15%)
Narrowing of the intervertebral foramen due to osteophytes, facet joint hypertrophy, thickening of the ligamentum flavum. More common in patients over 60 years.
Spondylolisthesis
Vertebral slippage leads to deformation of the foraminal opening and root compression.
Inflammation and edema
Even without significant mechanical compression, inflammatory mediators (TNF-alpha, IL-1, PGE2) released by the damaged disc cause chemical irritation and edema of the root.
Clinical Presentation by Levels
Cervical radiculopathy
C5 (disc C4-C5)
Pain in the shoulder, weakness of the deltoid muscle (difficulty raising the arm). Numbness on the outer surface of the shoulder. Decreased biceps reflex.
C6 (disc C5-C6)
Pain along the outer surface of the forearm. Numbness of the thumb and index finger. Weakness of the biceps and radial wrist extensor.
C7 (disc C6-C7)
The most common cervical radiculopathy. Pain along the posterior surface of the forearm. Numbness of the middle finger. Triceps weakness.
C8 (disc C7-T1)
Numbness of the ring and little fingers. Weakness of the small hand muscles. Often confused with cubital tunnel syndrome.
Lumbar radiculopathy
L4 (disc L3-L4)
Pain along the anterior surface of the thigh and medial shin. Weakness of the quadriceps muscle (difficulty extending the knee, climbing stairs). Decreased knee reflex.
L5 (disc L4-L5)
The most common lumbar radiculopathy. Pain along the outer surface of the thigh and shin, dorsum of the foot. Weakness of great toe and foot extension (foot drop in severe cases).
S1 (disc L5-S1)
Pain along the back of the thigh, calf, and outer foot. Weakness of plantar flexion (difficulty standing on tiptoes). Decreased Achilles reflex.
Severity Grades of Radiculopathy
Irritative (Irritation)
Pain and sensory disturbances only (numbness, paresthesias). Reflexes normal or mildly decreased. Muscle strength preserved. Optimal stage for MIBRAR® treatment.
Compressive (Compression)
Pain + numbness + muscle weakness. Decreased reflexes. EMG shows reduced conduction velocity and denervation. Active treatment required to prevent muscle atrophy.
Paralytic
Marked muscle weakness or paralysis, absent reflexes. EMG shows axonal degeneration. Indication for urgent intervention (MIBRAR® or surgery depending on the situation).
Diagnosis
MRI
Primary diagnostic method. Visualizes disc herniation/protrusion, stenosis, and nerve root condition. Sagittal and axial images. For cervical radiculopathy, myelopathy must be excluded.
EMG
Electromyography confirms radiculopathy, determines level, and assesses severity (demyelination vs. axonopathy). Prognostically important: axonal injury has longer recovery time.
Clinical Tests
Lasègue test (SLR) for lumbar radiculopathy. Spurling test for cervical radiculopathy. Muscle testing using MRC scale. Dermatome sensory mapping.
Radiculopathy Treatment with MIBRAR®
MIBRAR® addresses three mechanisms of radiculopathy: eliminates compression, reduces inflammation, and promotes nerve regeneration.
1. Compression Relief
Intradiscal injection of CGF + Lipogems® initiates disc regeneration. As the annulus fibrosus recovers, the disc bulge decreases, freeing the nerve root.
2. Anti-inflammatory Therapy
Perineural injection of CGF to the inflamed nerve root. Suppression of TNF-alpha, IL-1, and PGE2. Reduction of nerve root edema. Effect is faster and more sustained than corticosteroid blocks.
3. Nerve Regeneration
NGF, BDNF, and GDNF from CGF and paracrine secretion from stem cells stimulate remyelination (nerve sheath recovery) and axonal growth. Restoration of sensation and strength.
Don't wait for nerve death
Prolonged compression leads to irreversible damage. Submit your MRI for free evaluation.
Submit MRI ImagesTreatment Results for Radiculopathy
MRI follow-up confirms nerve root decompression and disc regeneration after the MIBRAR® procedure.

MIBRAR Case: female, 54 years
Diagnosis: S1 radiculopathy due to central L5/S1 herniation measuring 13.27 mm. Axial MRI — roots compressed bilaterally, right leg paraparesis.
Result at 11 months: herniation regression, root decompression, canal widening. Sensation restored, shooting pain resolved.
View case study →
MIBRAR Case: female, 43 years
Coronal MRI: green arrows indicate neuroforaminal stenosis L4/L5 and L5/S1 with root compression. Post-nucleotomy condition.
Result at 18 months: neuroforaminal widening, free root passage at both levels. Complete sensation recovery.
View case study →Questions about Radiculopathy
"Radiculitis" is an outdated term implying nerve root inflammation. The modern term is radiculopathy (nerve root damage). The cause is usually mechanical (compression) rather than inflammatory.
Yes, in 85-90% of cases. MIBRAR® eliminates compression through disc regeneration, reduces nerve root inflammation, and promotes nerve tissue recovery. Surgery is only indicated for cauda equina syndrome or progressive paralysis.
Pain decreases within 2-4 weeks. Sensation recovers within 2-6 weeks. Muscle strength improves within 1-3 months. Complete nerve regeneration takes 6-12 months in severe injuries.
Epidural corticosteroid injections provide temporary relief (2-6 weeks). They do not address the underlying cause. MIBRAR® solves the problem at the root: it regenerates the disc and restores nerve function.
Spine MRI — essential (shows the cause). EMG — confirms radiculopathy and determines severity. X-ray — when spinal instability or spondylolisthesis is suspected.