
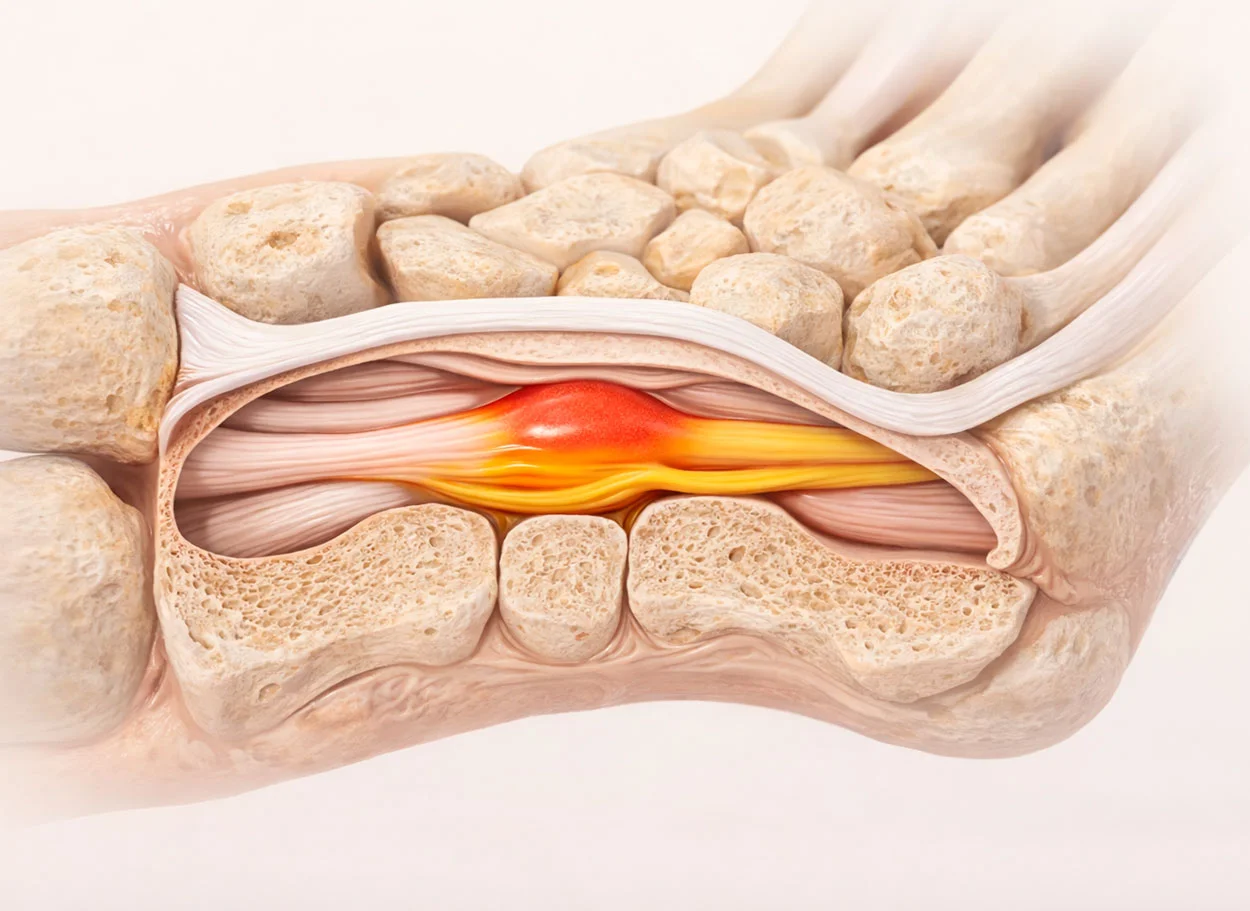
What is carpal tunnel syndrome?
Carpal tunnel syndrome (CTS) is a compressive neuropathy of the median nerve in the area of the carpal (wrist) tunnel. The tunnel is formed by the carpal bones and the transverse carpal ligament (retinaculum flexorum). Nerve compression occurs due to thickening of the ligament or swelling of the tunnel contents.
CTS is the most common compressive neuropathy, affecting 3-6% of the adult population. Women are affected more often (ratio 3:1). Bilateral involvement occurs in 50-60% of patients.
Causes:
- Prolonged computer work (typing, mouse use)
- Manual labor with repetitive movements
- Pregnancy and hormonal changes
- Diabetes mellitus, hypothyroidism
- Rheumatoid Arthritis
- History of wrist injuries
Severity grades:
- Mild — intermittent numbness, especially at night
- Moderate — constant numbness, reduced sensation, pain
- Severe — thenar muscle atrophy, loss of grip strength, permanent sensory loss
Facts about CTS
- ICD-10: G56.0
- Prevalence: 3-6% adults
- Gender: women 3 times more often
- Bilateral: 50-60% cases
- Surgeries: 500 000+/year in USA
- Recurrence after surgery: 3-25%
Symptoms of carpal tunnel syndrome
Early signs
- Numbness and tingling in fingers I-III at night
- Need to "shake out" the hand for relief
- Sensation of finger swelling in the mornings
- Tingling during computer work
Progression
- Constant finger numbness
- Pain in hand and wrist
- Reduced fingertip sensation
- Clumsiness (dropping objects)
- Thumb weakness
Severe Stage
- Thenar muscle atrophy (at the base of the thumb)
- Loss of pinch and grip strength
- Inability to button a shirt
- Loss of tactile sensation
- Chronic pain
Surgery vs MIBRAR®
| Criterion | Surgical Decompression | Corticosteroid Injections | MIBRAR® |
|---|---|---|---|
| Principle | Transverse carpal ligament release | Reducing swelling with medications | Nerve regeneration + biological decompression |
| Anesthesia | Local / regional | None | No anesthesia |
| Ligament Preservation | ❌ Ligament permanently severed | ✅ Preserved | ✅ Preserved — decompression without incision |
| Grip Strength | Reduced for 3-6 months | No change | No reduction |
| Nerve Regeneration | ❌ Decompression only | ❌ None | ✅ Stem cells restore the nerve |
| Both Hands at Once | ❌ One at a time | Possible | ✅ Yes |
How MIBRAR® treats Carpal Tunnel Syndrome
Ultrasound Diagnosis
Sono Control Arm™ visualizes the median nerve, measures its cross-sectional area (>10 mm² = compression), and assesses the condition of tendons and the carpal tunnel ligament.
Biomaterial Preparation
CGF — anti-inflammatory factors and neurotrophic growth factors (NGF, BDNF). Lipogems® — stem cells with neuroregenerative potential.
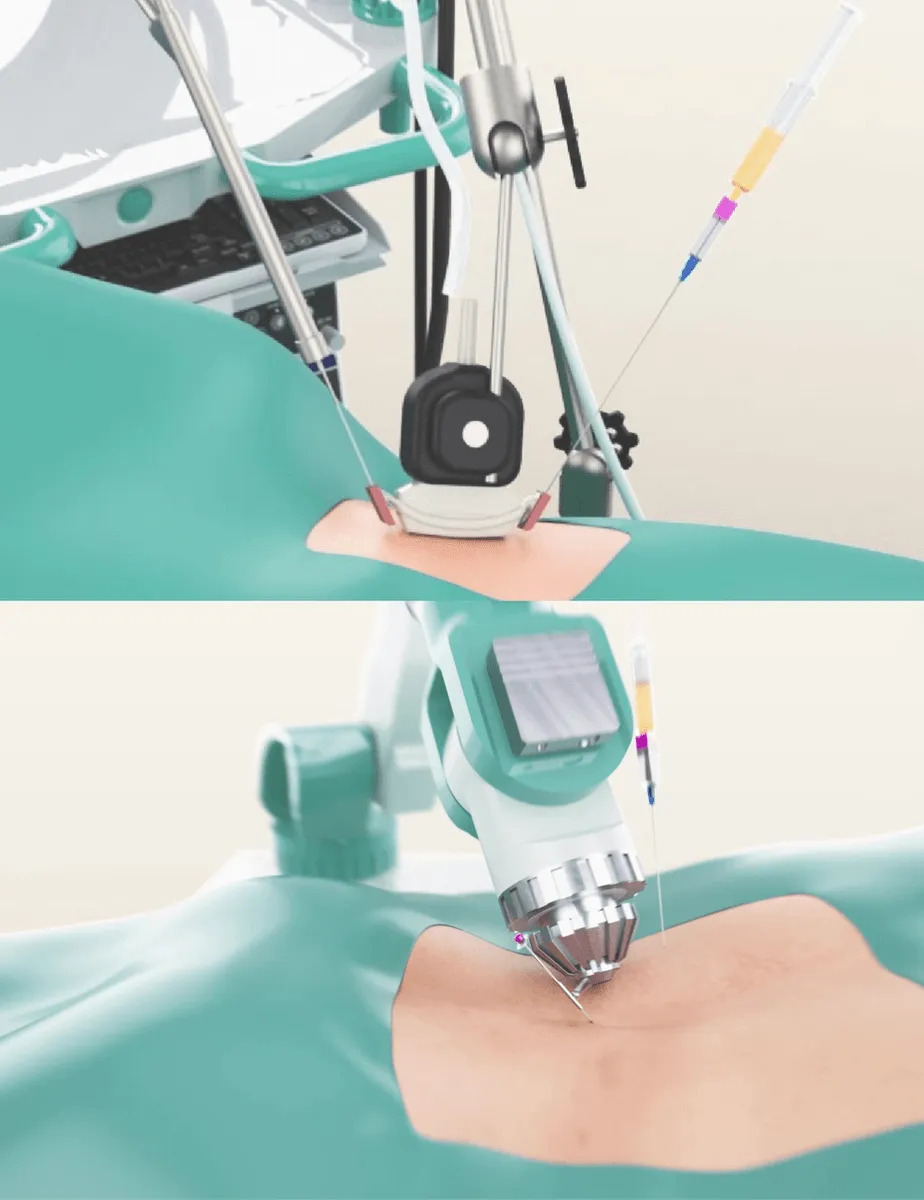
Targeted Injection
Under ultrasound guidance, concentrates are injected into the carpal tunnel — around the median nerve, into the thickened transverse carpal ligament, and into the area of maximum compression. Hydrodissection technique releases the nerve.
Neuroregeneration
Stem cells restore the myelin sheath of the damaged nerve, reduce ligament fibrosis, and relieve swelling. Result — elimination of compression and restoration of nerve conduction.
Why MIBRAR® is effective for CTS
Surgery for CTS severs the ligament — this relieves pressure but does not restore the damaged nerve. MIBRAR® addresses both problems: ultrasound-guided hydrodissection frees the nerve without incision, while stem cells trigger neuroregeneration — restoration of the myelin sheath and axons. Neurotrophic factors (NGF, BDNF) from CGF stimulate nerve fiber growth. Result — not only decompression but also restoration of nerve conduction.
MIBRAR® Method Advantages
95% of interventions covered
MIBRAR® covers up to 95% of all spinal neurosurgery and orthopedic operations.
No anesthesia or incisions
Outpatient treatment via 0.3-1.5 mm puncture. No general anesthesia or hospitalization.
No age restrictions
Regeneration at any age. Safe for chronic conditions and anesthesia intolerance.
Rapid improvement
Concentrates have analgesic and anti-inflammatory properties. Relief within days.
Multiple zones at once
Simultaneous treatment of multiple discs or joints in one procedure.
Home the same day
No crutches, braces or rehabilitation needed. MRI follow-up at 8-16 weeks.
MIBRAR® Technology
Cyber Navi Hand™
Intraoperative robotic navigation system. Provides precise access to deep structures with 1 mm and 1 degree accuracy.

Sono Control Arm™
Device for intervention under sonographic control. Eliminates open surgeries with real-time visual monitoring.