
What is chondromalacia?
Chondromalacia patellae (patellofemoral syndrome) — softening and destruction of the cartilage covering the posterior surface of the patella (kneecap). The cartilage loses its smoothness, becomes rough and friable, leading to pain, crepitus, and inflammation during movement.
This is one of the most common causes of anterior knee pain, especially in young people and athletes. Chondromalacia occurs in 25% of all patients with knee pain.
Stages of chondromalacia (Outerbridge classification):
- Stage I — cartilage softening, swelling. Cartilage can be compressed with a finger
- Stage II — superficial cracks and fibrillation (fraying)
- Stage III — deep cracks, destruction of more than 50% of cartilage thickness
- Stage IV — complete cartilage destruction, exposure of subchondral bone
Causes:
- Patellar maltracking — displacement of the patella during movement
- Overload — running, squatting, jumping
- Weakness of the vastus medialis obliquus (VMO)
- Flat feet — disruption of lower limb biomechanics
- Trauma — direct blow to the patella, dislocation
Facts about chondromalacia
- ICD-10: M22.4
- Frequency: 25% of patients with knee pain
- Age: 15-40 years (more common in young people)
- Gender: women 2 times more often
- Issue: patellar cartilage is the thickest in the body (up to 7 mm)
Symptoms of chondromalacia
Typical complaints
- Pain in the anterior knee
- Worsens when climbing and descending stairs
- Pain when standing up after prolonged sitting («movie theater sign»)
- Crepitus (crunching, creaking) when bending the knee
- Pain when squatting
Progression
- Increasing pain with any load
- Swelling around the patella
- Quadriceps muscle weakness
- Limited knee flexion
- Progression to patellofemoral osteoarthritis
When to See a Doctor
- Pain persists for more than 2-3 weeks
- Pain interferes with daily activities
- Swelling or knee locking develops
- Physical therapy and NSAIDs are not helping
- Knee crepitus worsens
How MIBRAR® Treats Chondromalacia
MRI Cartilage Assessment
MRI of the knee joint determines the stage of chondromalacia, localization and depth of cartilage damage, and the condition of the patellofemoral joint.
Obtaining Concentrates
From blood — CGF with chondrogenic growth factors. From adipose tissue — Lipogems® with mesenchymal stem cells capable of differentiating into chondrocytes.
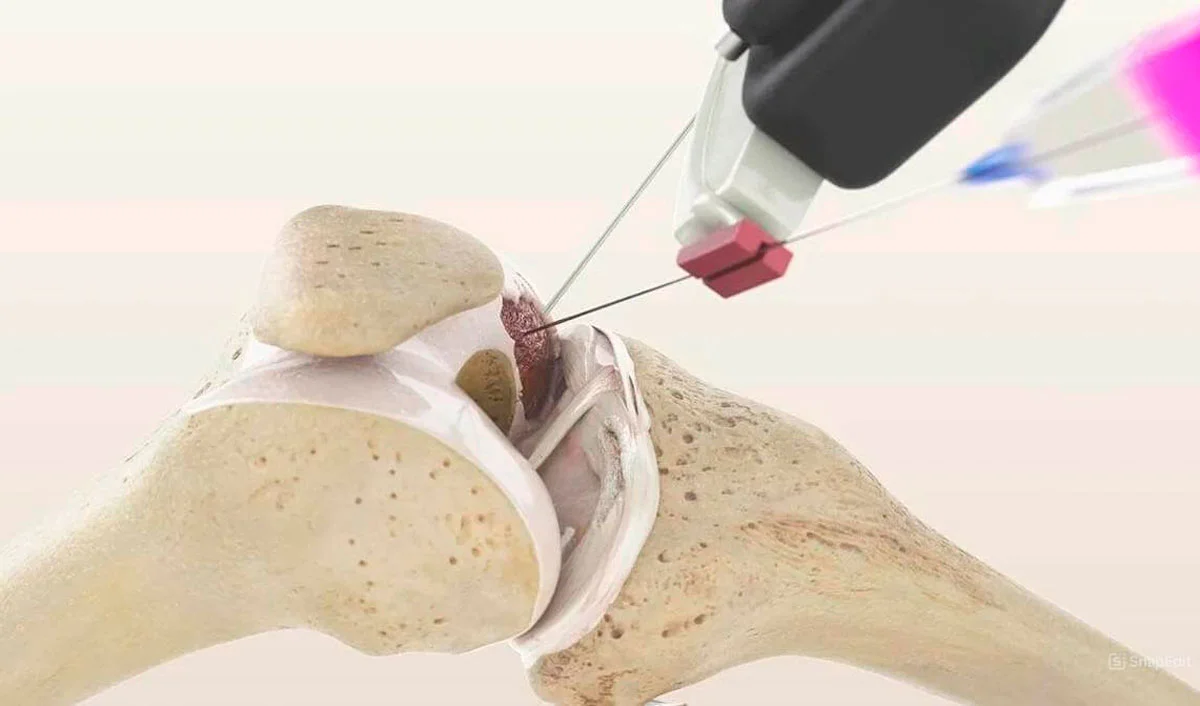
Intra-articular Injection
Under Sono Control Arm™ guidance, concentrates are injected into the knee joint cavity with emphasis on the patellofemoral compartment — directly to the damaged patellar cartilage.
Cartilage Regeneration
Stem cells differentiate into chondrocytes and restore the damaged cartilage surface. Anti-inflammatory factors reduce synovitis. The cartilage regains smoothness — crepitus and pain resolve.
Treatment Results for Knee Cartilage
Follow-up MRI confirms regeneration of knee joint cartilage tissue after MIBRAR® — without arthroscopy or surgical intervention.

MIBRAR Case: Male, 49 years
Diagnosis: Grade IV gonarthrosis with complete destruction of the medial condylar cartilage and subchondral osteonecrosis. Sagittal MRI (image 7) — cartilage coating absent, bone exposed.
Result after 18 months (image 8): restoration of condylar cartilage coating, normalization of subchondral bone structure. Lipogems® stem cells differentiated into chondrocytes and created a new cartilage matrix.
View case study →
MIBRAR Case: Male, 56 years
Sagittal MRI (image 5): before treatment — damage to the cartilage surface of the femoral condyle and meniscus tear. Green oval marks the pathology zone.
After 4 weeks (image 6): improvement of the cartilage surface structure, beginning of meniscus regeneration. MIBRAR® restores cartilage at the cellular level — unlike arthroscopy, which only smooths the damaged surface.
View case study →MIBRAR® Method Advantages
95% of interventions covered
MIBRAR® covers up to 95% of all spinal neurosurgery and orthopedic operations.
No anesthesia or incisions
Outpatient treatment via 0.3-1.5 mm puncture. No general anesthesia or hospitalization.
No age restrictions
Regeneration at any age. Safe for chronic conditions and anesthesia intolerance.
Rapid improvement
Concentrates have analgesic and anti-inflammatory properties. Relief within days.
Multiple zones at once
Simultaneous treatment of multiple discs or joints in one procedure.
Home the same day
No crutches, braces or rehabilitation needed. MRI follow-up at 8-16 weeks.
MIBRAR® Technology
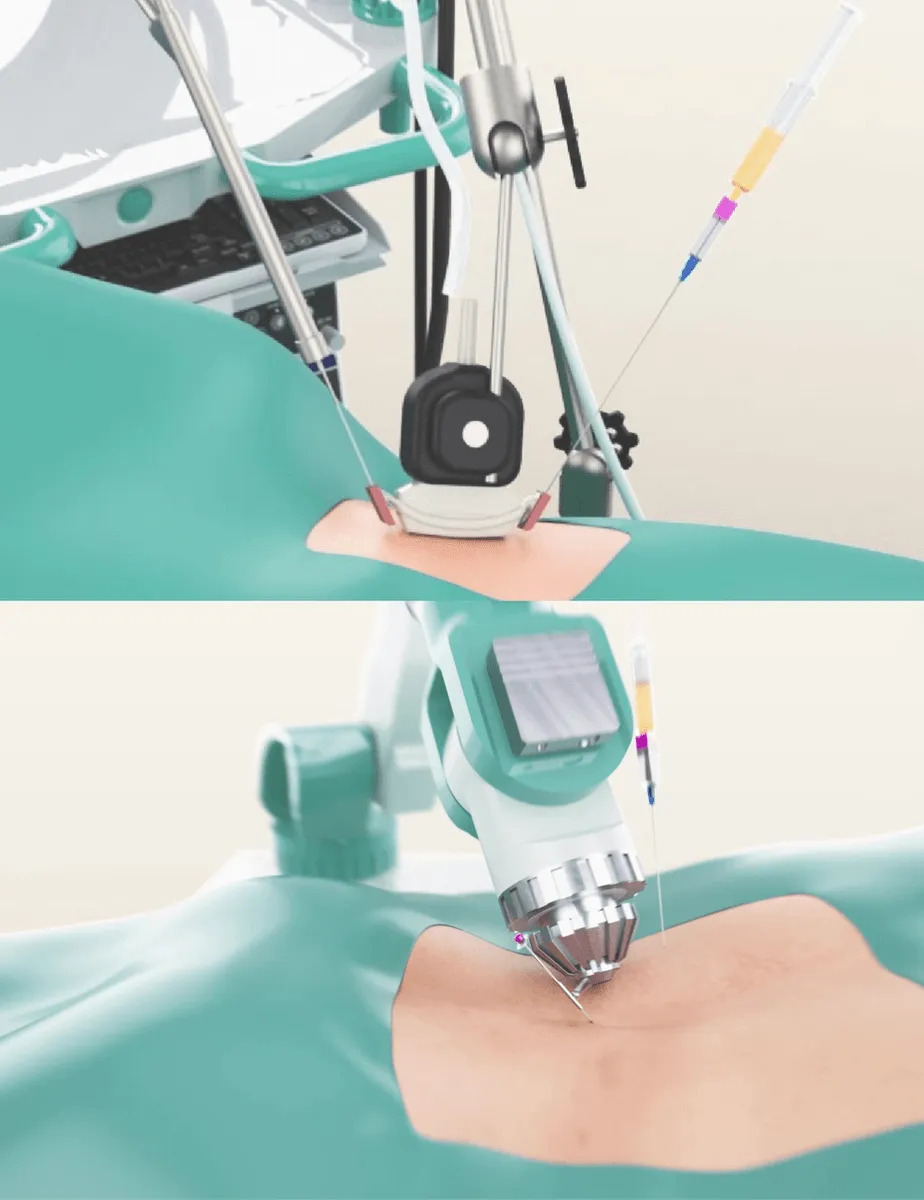
Cyber Navi Hand™
Intraoperative robotic navigation system. Provides precise access to deep structures with 1 mm and 1 degree accuracy.

Sono Control Arm™
Device for intervention under sonographic control. Eliminates open surgeries with real-time visual monitoring.