
What is a cruciate ligament injury?
Cruciate ligaments (anterior — ACL and posterior — PCL) are the main stabilizers of the knee joint. They prevent displacement of the tibia relative to the femur. ACL tear is one of the most common sports injuries, with approximately 200 000 cases occurring worldwide annually.
Traditionally, ACL tears are treated with arthroscopic reconstruction — the ligament is replaced with a graft from the patient's own tendon (hamstring or quadriceps). However, 10-25% of reconstructions fail, and tendon harvesting weakens the donor muscle.
Degrees of injury:
- Grade I (sprain) — microfiber tears, ligament intact, mild instability
- Grade II (partial tear) — up to 50% of fibers damaged, moderate instability
- Grade III (complete tear) — ligament fully torn, significant instability
Risk factors:
- Contact sports (soccer, basketball, martial arts)
- Sudden stops and turns (skiing, tennis)
- Female sex (2-8 times higher risk due to anatomy)
- Weakness of knee stabilizer muscles
Facts about ACL tears
- ICD-10: S83.5
- Frequency: 200 000 cases/year worldwide
- Age: 15-45 years
- Sex: women 2-8 times more often
- Reconstruction failures: 10-25%
Symptoms of ACL tear
Acute tear
- Sudden pain and "pop" at the moment of injury
- Rapid swelling (hemarthrosis within the first hours)
- Inability to continue activity
- Sensation of "knee dislocation"
- Instability when walking
Chronic ACL deficiency
- Sensation of "knee giving way"
- Instability when running, descending stairs
- Periodic swelling after activity
- Quadriceps muscle atrophy
- Progressive meniscus and cartilage damage
Consequences without treatment
- Chronic knee instability
- Meniscus tears (secondary)
- Accelerated osteoarthritis development
- Inability to participate in sports
- Reduced quality of life
How MIBRAR® treats ligament injuries
MIBRAR® is most effective for partial tears (Grade I-II) and acute injuries. In complete ruptures, it can be used as a complement to surgical reconstruction to accelerate graft integration.
MRI Diagnostics
MRI of the knee joint determines the degree of ligament damage, presence of associated meniscus and cartilage injuries. The feasibility of regenerative treatment is assessed.
Obtaining Concentrates
From blood — CGF with connective tissue growth factors. From adipose tissue — Lipogems® with stem cells capable of differentiating into tenocytes and fibrocytes — ligament tissue cells.
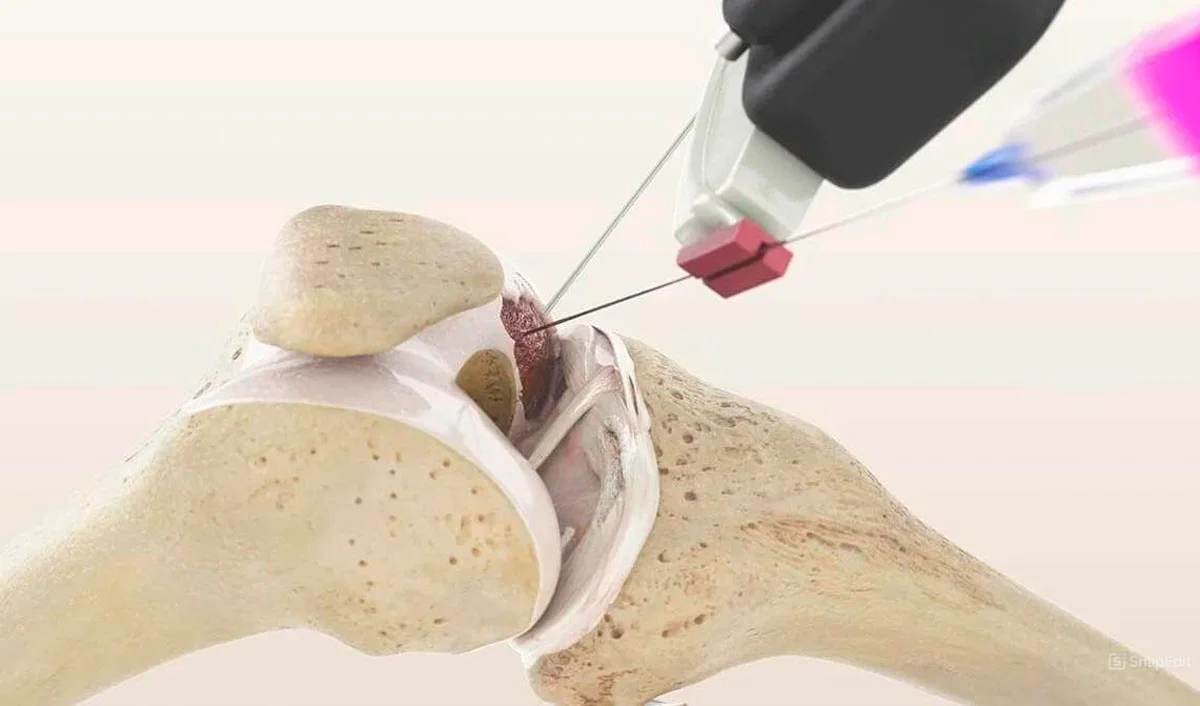
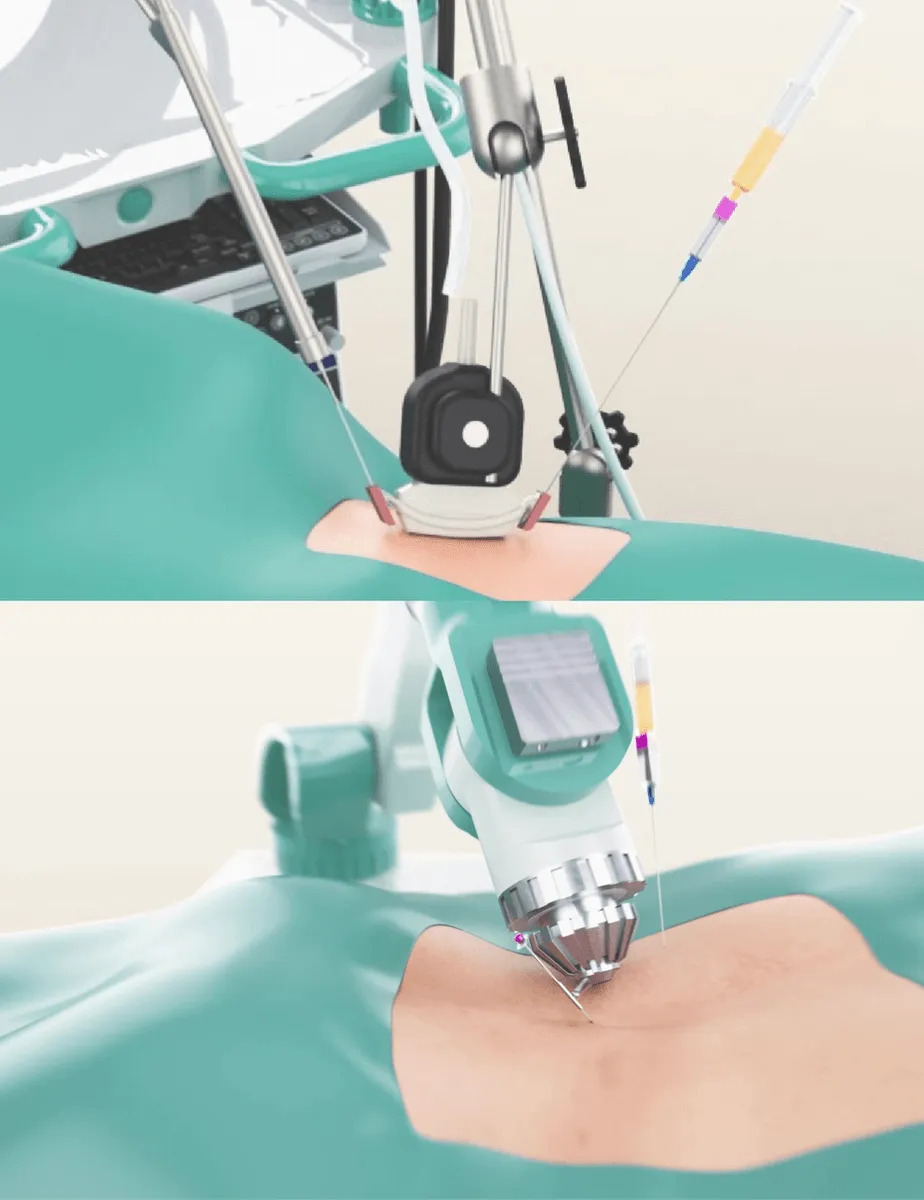
Injection into the Injury Site
Under ultrasound guidance with Sono Control Arm™, concentrates are injected directly into the damaged ligament. Damaged menisci and cartilage are treated simultaneously (if necessary).
Ligament Regeneration
Stem cells differentiate into tenocytes and synthesize Type I collagen — the main ligament component. Growth factors stimulate angiogenesis and formation of new fibers. The ligament strengthens and restores its stabilizing function.
ACL Reconstruction vs MIBRAR®
| Criterion | Arthroscopic Reconstruction | MIBRAR® |
|---|---|---|
| Principle | Ligament replacement with graft | Regeneration of native ligament |
| Anesthesia | General / spinal | No anesthesia |
| Donor Site | Tendon harvest (muscle weakening) | None — autologous cells from blood and fat |
| Rehabilitation | 6-9 months, crutches 4-6 weeks | Several weeks |
| Return to Sports | 9-12 months | 8-16 weeks (for partial tear) |
| Indication | Complete rupture + high demands | Partial tear, acute injury |
Treatment Results for the Knee Joint
Sagittal MRI before and 18 months after MIBRAR® demonstrates regeneration of knee joint structures — including ligaments, menisci, and articular cartilage.

MIBRAR Case: Male, 49 years
Diagnosis: Grade IV gonarthrosis with osteonecrosis of the medial condyle and subchondral edema. Sagittal MRI (image 3) — severe destruction of articular surfaces with involvement of the ligamentous apparatus.
Result after 18 months: regeneration of cartilaginous and ligamentous structures (image 4). Restoration of joint space, elimination of subchondral edema. Complete restoration of mobility.
View case study →
Same Patient — Different Sagittal Slice
Sagittal MRI (image 7): before treatment — extensive zone of osteonecrosis and destruction of joint structures. Cruciate ligaments visualized in the zone of the damaged joint.
After 18 months (image 8): restoration of condylar bone tissue, normalization of articular surfaces. MIBRAR® regenerates all knee joint structures simultaneously — cartilage, ligaments, menisci, subchondral bone.
View case study →MIBRAR® Method Advantages
95% of interventions covered
MIBRAR® covers up to 95% of all spinal neurosurgery and orthopedic operations.
No anesthesia or incisions
Outpatient treatment via 0.3-1.5 mm puncture. No general anesthesia or hospitalization.
No age restrictions
Regeneration at any age. Safe for chronic conditions and anesthesia intolerance.
Rapid improvement
Concentrates have analgesic and anti-inflammatory properties. Relief within days.
Multiple zones at once
Simultaneous treatment of multiple discs or joints in one procedure.
Home the same day
No crutches, braces or rehabilitation needed. MRI follow-up at 8-16 weeks.
MIBRAR® Technology
Cyber Navi Hand™
Intraoperative robotic navigation system. Provides precise access to deep structures with 1 mm and 1 degree accuracy.

Sono Control Arm™
Device for intervention under sonographic control. Eliminates open surgeries with real-time visual monitoring.