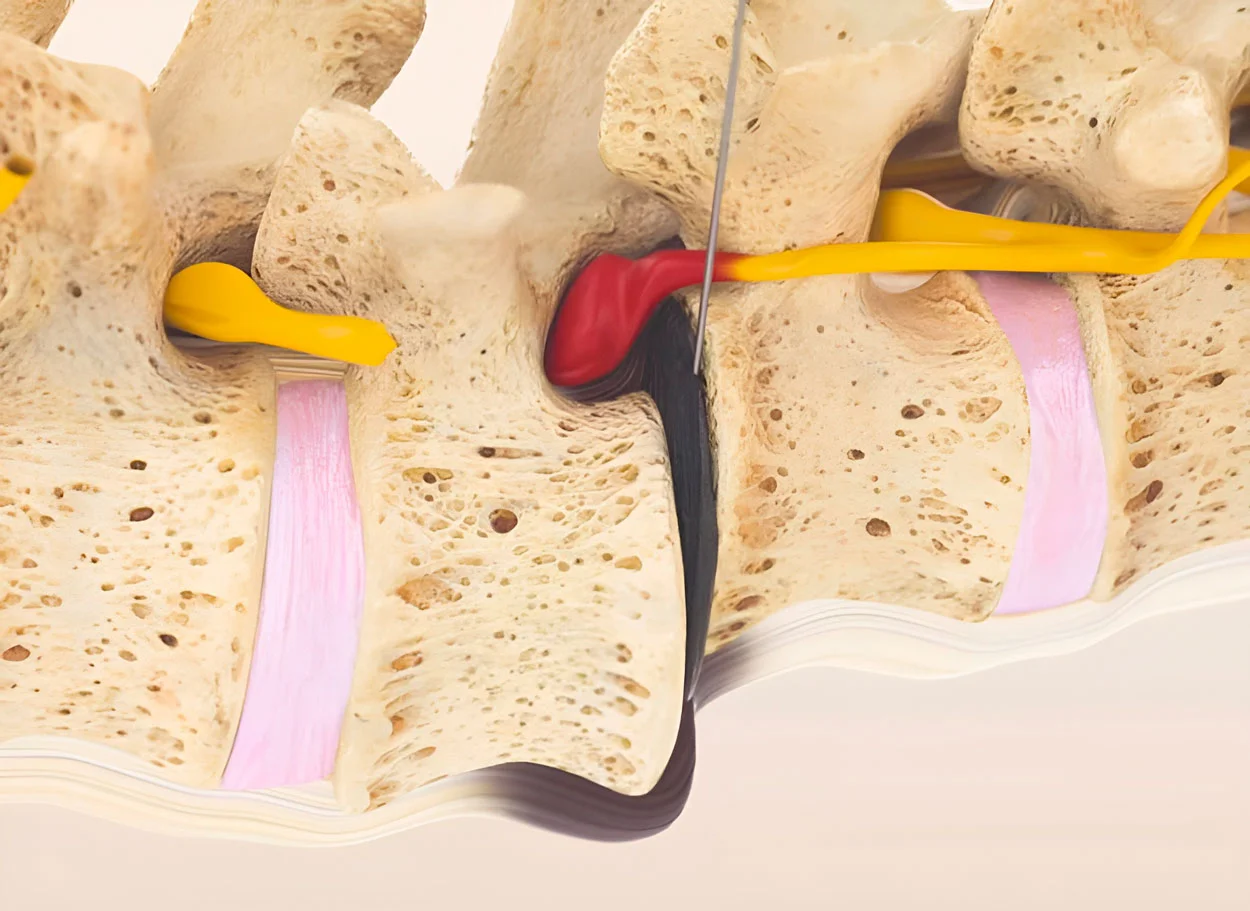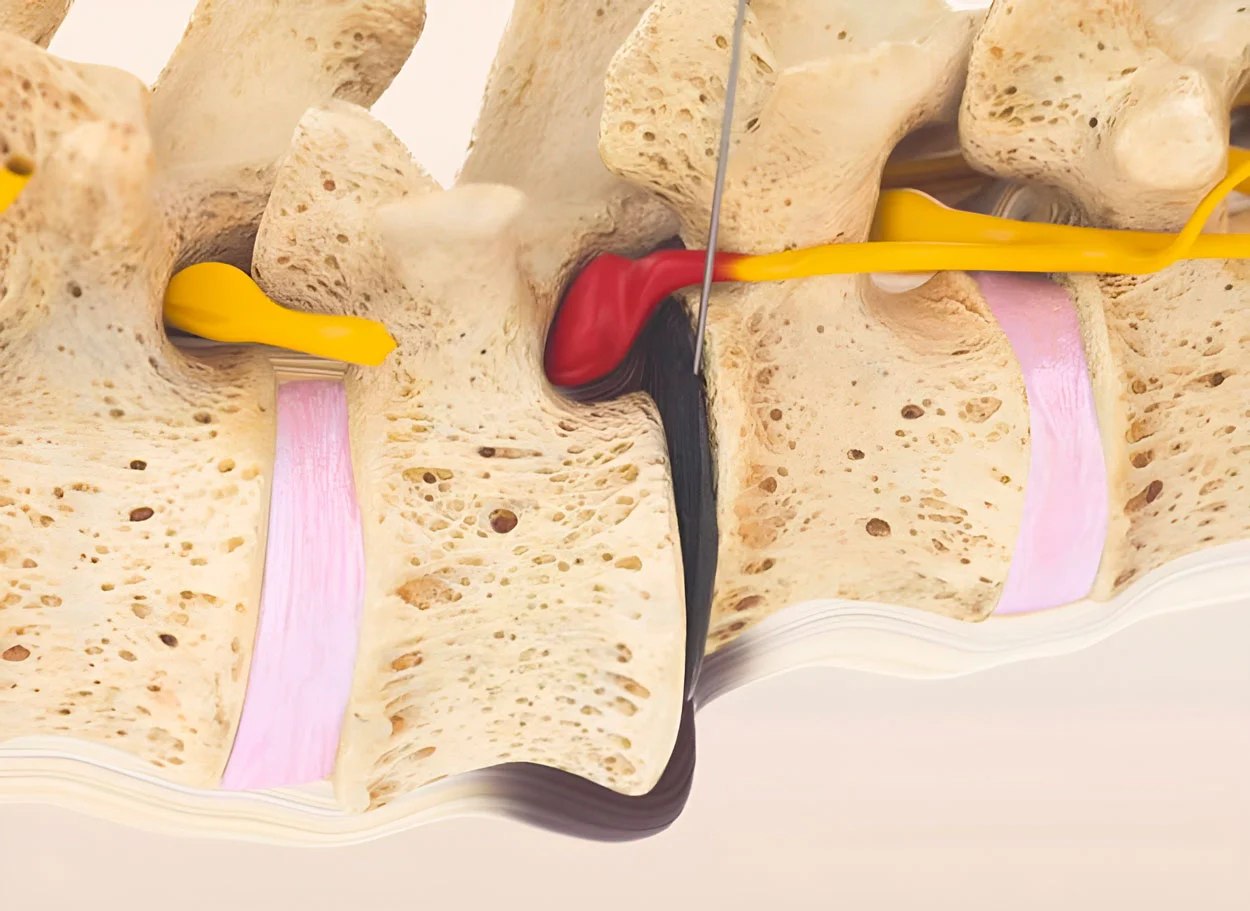
What is spondylolisthesis?
Spondylolisthesis is the slippage of one vertebra relative to another. It most commonly slips forward (anterolisthesis), less often backward (retrolisthesis). This leads to instability of the spinal segment, narrowing of the spinal canal, and compression of neural structures.
Spondylolisthesis occurs in 5-7% of the population, most frequently at the L4-L5 and L5-S1 levels. In athletes (gymnasts, weightlifters), the prevalence reaches 15-40%.
Degrees of slippage (Meyerding):
- Grade I — slippage up to 25% of the vertebral body width
- Grade II — slippage 25-50%
- Grade III — slippage 50-75%
- Grade IV — slippage more than 75%
- Spondyloptosis — complete slippage
Types of spondylolisthesis:
- Isthmus — pars defect (spondylolysis), most common
- Degenerative — due to facet joint osteoarthritis, more common in the elderly
- Dysplastic — congenital anomaly
- Traumatic — after pars fracture
Facts about spondylolisthesis
- ICD-10: M43.1
- Prevalence: 5-7% of the general population
- In athletes: 15-40%
- Location: 90% at L4-L5 and L5-S1 levels
- Peak: young athletes and elderly (degenerative)
Symptoms of spondylolisthesis
Main symptoms
- Low back pain worsening with loading
- Sensation of instability with movement
- Stiffness and limited extension
- Paravertebral muscle spasm
- Palpable "step-off"
Neurological manifestations
- Leg-referred pain (sciatica)
- Neurogenic claudication
- Numbness and weakness in legs
- Reflex impairment
- In severe cases — cauda equina syndrome
Features
- Pain worsens with prolonged standing
- Relief when bending forward
- Characteristic "waddling" gait (in pronounced cases)
- Lumbar hyperlordosis
- Trunk shortening (in III-IV degree)
Spinal Fusion vs MIBRAR®
| Criterion | Spinal Fusion (Fixation) | Conservative Treatment | MIBRAR® |
|---|---|---|---|
| Principle | Fusion of vertebrae with metal constructs | Brace, physical therapy, pain relief | Regeneration of ligaments and discs, biological stabilization |
| Anesthesia | General | None | No anesthesia |
| Hospitalization | 5-10 days | None | None — home the same day |
| Spinal Mobility | ❌ Lost in the fixation zone permanently | ✅ Preserved | ✅ Fully preserved |
| Adjacent Segments | Overload → degeneration in 5-10 years | No effect | Not affected — no rigid fixation |
| Rehabilitation | 3-6 months, restrictions for a year | Ongoing | Several days |
How MIBRAR® treats spondylolisthesis
3D diagnosis of displacement
Functional X-rays and MRI are analyzed by the Cyber Navi Hand™ system. Degree of displacement, condition of discs, ligaments, and facet joints at the level of listhesis and adjacent segments are determined.
Obtaining biomaterial
CGF with growth factors stimulating regeneration of ligaments and cartilage is obtained from blood. Lipogems® with stem cells for restoration of damaged structures is obtained from adipose tissue.
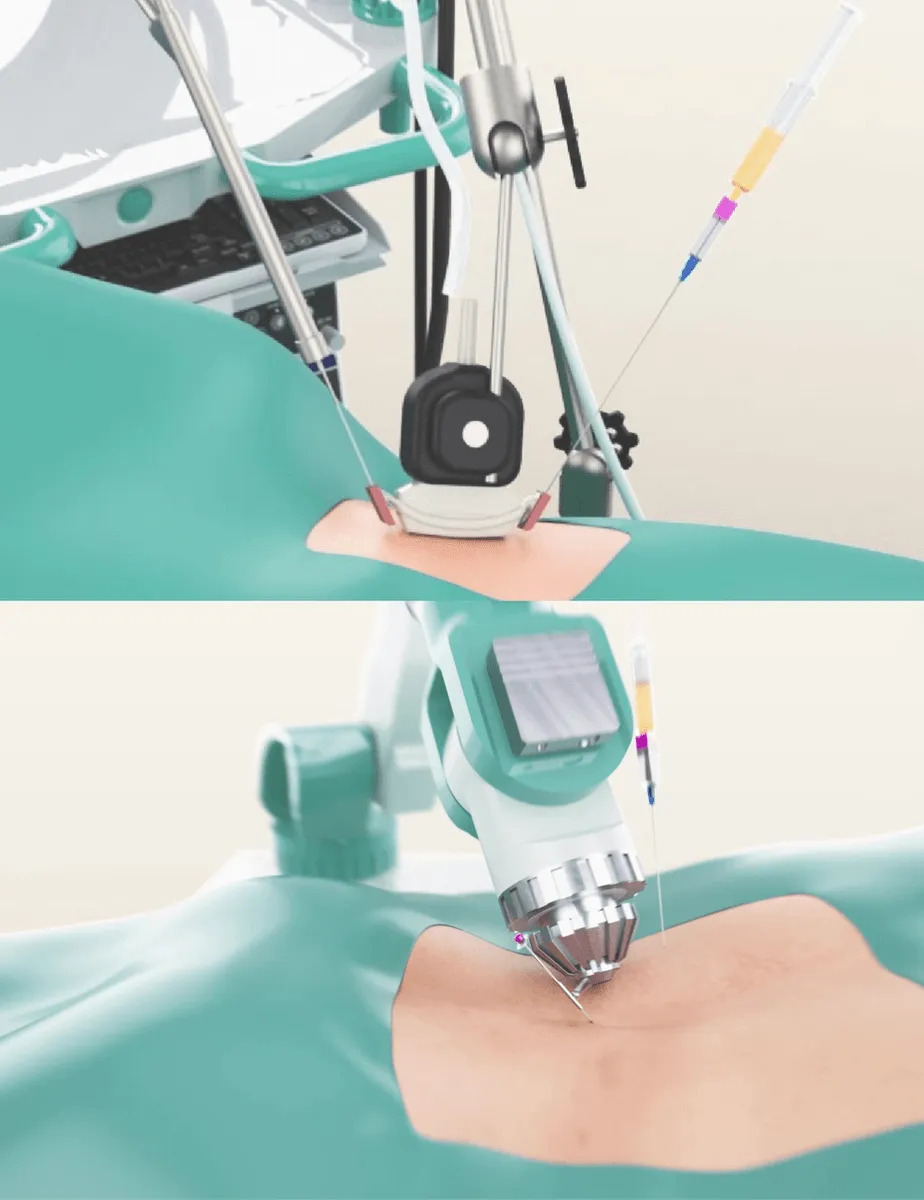
Complex injection
Concentrates are injected into the damaged disc, weakened ligaments (anterior and posterior longitudinal, interspinous), facet joints, and paravertebral muscles. This creates a biological corset.
Biological stabilization
Stem cells strengthen the ligamentous apparatus, restore disc height, reduce inflammation of facet joints. Result — segment stabilization without loss of mobility.
Why MIBRAR® is effective for spondylolisthesis
In spondylolisthesis, the main problem is segmental instability. Traditional medicine addresses it with rigid fixation (spinal fusion), but this creates new problems: loss of mobility and overload of adjacent segments. MIBRAR® creates biological stabilization — strengthens the natural stabilizers of the spine.
Mechanism of biological stabilization:
- Strengthening of the ligamentous apparatus — growth factors stimulate collagen synthesis in longitudinal ligaments, interspinous and supraspinous ligaments, increasing their tear strength
- Disc regeneration — restoration of disc height and elasticity in the listhesis zone improves load distribution and reduces pathological displacement
- Treatment of facet joints — reduction of osteoarthritis and inflammation of facet joints, which are key stabilizers of the posterior support complex
- Anti-inflammatory effect — reduction of chronic inflammation in the instability zone, which accelerates tissue destruction
Result: the spinal segment is stabilized biologically — ligaments become stronger, the disc regenerates, joints stop inflaming. Mobility is fully preserved, unlike spinal fusion.
MIBRAR® for Spondylolisthesis
- No metal implants — biological stabilization
- Mobility preserved — no segment blockage
- No adjacent segment syndrome
- Comprehensive effect — ligaments + disc + joints
- No general anesthesia — outpatient
Treatment Results for Spondylolisthesis
MRI follow-up confirms vertebral stabilization and disc regeneration after the MIBRAR® procedure — without surgery or fixation.

MIBRAR Case: Female, 54 years
Diagnosis: Right-sided scoliosis, ventral spondylolisthesis L4 with 6 mm slippage, central L5/S1 herniation of 14 mm, spinal canal stenosis. Right leg paraparesis — unable to stand or walk independently.
Result at 11 months: Herniation regression, vertebral stabilization. After 2 weeks — all symptoms resolved. After 6 weeks — active sports. No symptom recurrence to date.
View case study →
Same patient — axial view
Axial MRI at L5/S1: 13.27 mm herniation (green arrow) with significant nerve root compression. Bilateral neuroforaminal stenosis.
At 11 months: Herniation regression, root decompression, spinal canal widening. MIBRAR® avoided the need for spinal fusion surgery.
View case study →
MIBRAR Case: Intradiscal MIBRAR® Procedure
Lateral fluoroscopy: two images show precise injection of CGF and Lipogems® into L3-L5 intervertebral discs. Red markers — vertebral body boundaries, green — disc injection points. Each disc is treated individually.
Significance: intradiscal regeneration restores disc height and elasticity, reducing pathological vertebral slippage. Unlike spinal fusion — segment mobility is fully preserved.
View case study →
Same Patient — Frontal View
AP fluoroscopy: two images show biomaterial injection into discs and facet joints at L3-S1 levels. Green markers indicate each injection point. Needle visible in the intervertebral disc.
MIBRAR® advantage: all damaged levels are treated in a single procedure — discs, facet joints, ligaments. Comprehensive biological stabilization instead of metal hardware.
View case study →MIBRAR® Method Advantages
95% of interventions covered
MIBRAR® covers up to 95% of all spinal neurosurgery and orthopedic operations.
No anesthesia or incisions
Outpatient treatment via 0.3-1.5 mm puncture. No general anesthesia or hospitalization.
No age restrictions
Regeneration at any age. Safe for chronic conditions and anesthesia intolerance.
Rapid improvement
Concentrates have analgesic and anti-inflammatory properties. Relief within days.
Multiple zones at once
Simultaneous treatment of multiple discs or joints in one procedure.
Home the same day
No crutches, braces or rehabilitation needed. MRI follow-up at 8-16 weeks.
MIBRAR® Technology
Cyber Navi Hand™
Intraoperative robotic navigation system. Provides precise access to deep structures with 1 mm and 1 degree accuracy.

Sono Control Arm™
Device for intervention under sonographic control. Eliminates open surgeries with real-time visual monitoring.