What is a Herniated Disc?
An intervertebral disc is a cartilaginous "cushion" between vertebrae, consisting of two components: the annulus fibrosus (dense outer layer made of collagen fibers) and the nucleus pulposus (gel-like core, 80% water). The disc acts as a shock absorber during walking, running, and lifting, and enables spinal mobility.
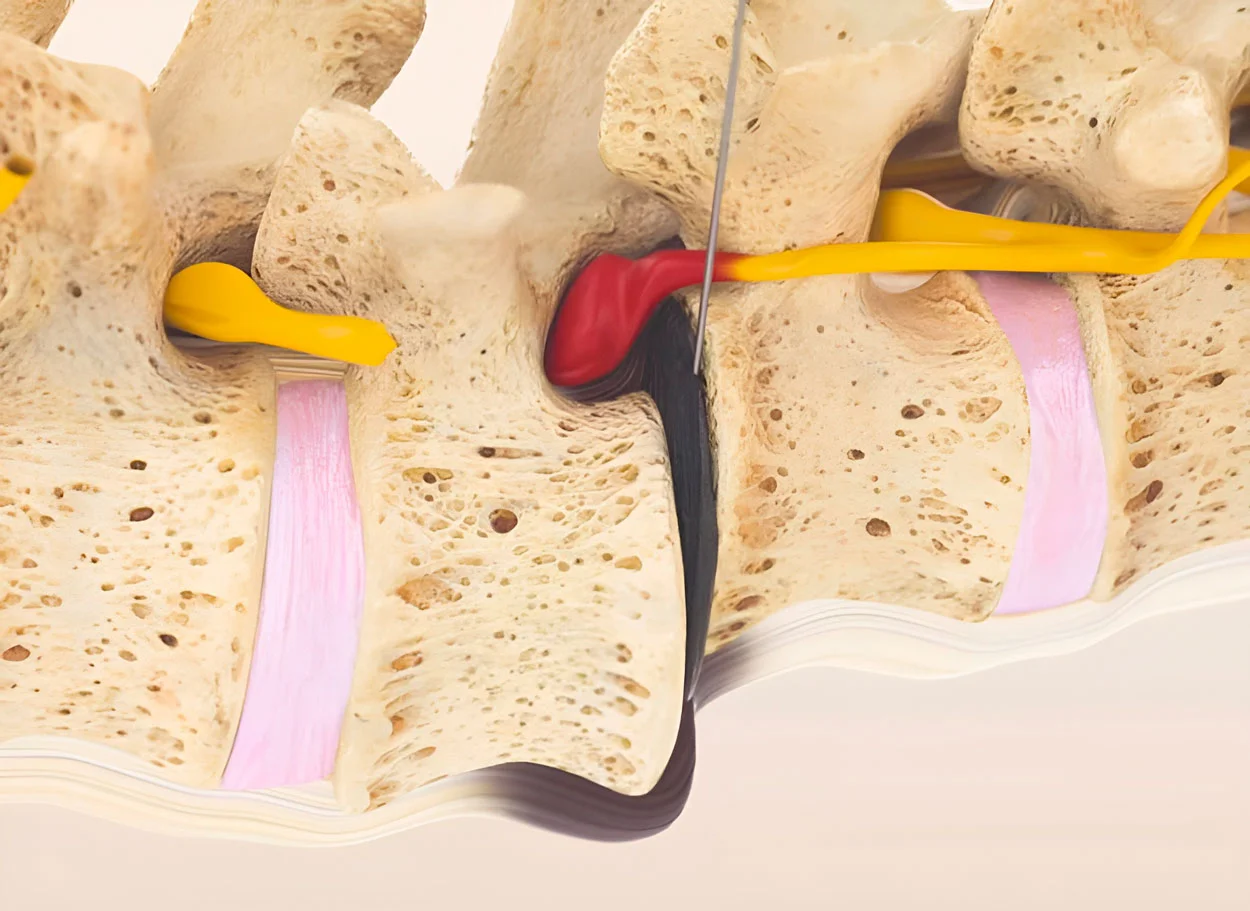
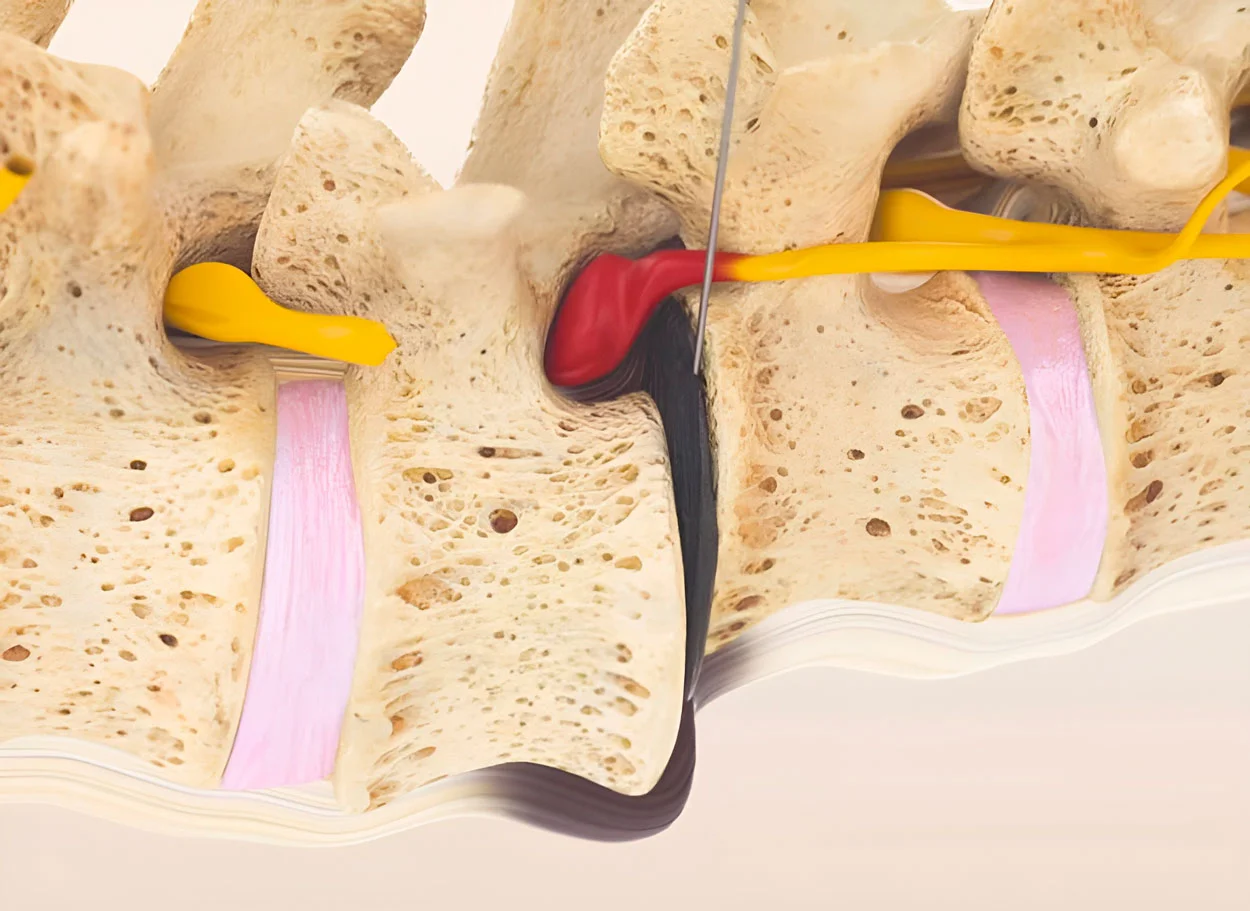
A herniated disc occurs when the annulus fibrosus is damaged (tear or crack), and the nucleus pulposus protrudes beyond the disc boundary. The protruding fragment can compress the spinal cord, nerve roots, and blood vessels, causing pain, numbness, and limited mobility.
According to KBV (Kassenärztliche Bundesvereinigung), musculoskeletal diseases are the #1 reason for doctor visits in Germany — affecting more than 36.7 million patients annually. Herniated disc is one of the most common conditions leading to chronic back pain and disability.
Stages of disc herniation:
- Disc degeneration — initial stage: disc loses water and elasticity, annulus fibrosus thins, microtears appear. Pain may be absent
- Disc protrusion (prolapse) — disc bulging 2-5 mm without annulus fibrosus rupture. May compress nerve roots
- Extrusion — annulus fibrosus rupture, part of nucleus pulposus extends outward while remaining connected to the disc
- Sequestration — nucleus pulposus fragment completely separates and migrates into the spinal canal. Most dangerous stage
Most common locations:
- L4-L5 — between 4th and 5th lumbar vertebrae (most common location — up to 45% of all hernias)
- L5-S1 — lumbosacral junction (up to 35% of cases)
- L3-L4 — upper lumbar level (up to 5%)
- C5-C6, C6-C7 — cervical spine (up to 10%)
- Thoracic region — thoracic spine (less than 5%, but often with severe symptoms)
Facts about Herniated Disc
- ICD-10: M51.1 (lumbar), M50.1 (cervical)
- Frequency: 5-20 cases per 1000 people per year
- Peak age: 30-50 years
- Location: 90% — lumbar spine
- Recurrence after surgery: up to 15-25%
- MIBRAR® success rate: 95% satisfaction
Causes and Risk Factors
Herniated disc is the result of a degenerative process that develops over years. The intervertebral disc receives nutrition not through blood vessels, but through diffusion — the seepage of nutrients from surrounding tissues during spine movement. This is why a sedentary lifestyle is one of the main factors of degeneration.
Main causes:
Degenerative changes
- Natural aging: with age, the disc loses up to 30% of its water content
- Osteochondrosis — degeneration of cartilage tissue
- Impaired metabolism in disc tissues
- Reduced elasticity of the annulus fibrosus
Mechanical factors
- Excessive physical stress on the spine
- Lifting heavy weights with improper technique
- Spinal injuries (car accidents, falls, sports)
- Prolonged forced posture (computer work)
Risk factors
- Excess weight (increased load on discs)
- Smoking (impairs blood supply to disc tissues)
- Genetic predisposition
- Occupational hazards (vibration, heavy labor)
- Sedentary lifestyle
Important to understand: herniated disc is not a "random event," but the result of a prolonged degenerative process. Traditional medicine offers surgical removal of the hernia, but this does not eliminate the cause — degeneration of the disc itself. This is why recurrences occur in 15-25% of cases after surgery. MIBRAR® works differently — the method initiates regeneration of damaged disc tissues, restoring its structure and function.
Symptoms of Herniated Disc
Symptoms depend on the location and size of the hernia, as well as the degree of compression of neural structures. A hernia as small as 3-4 mm can cause significant pain if unfavorably positioned relative to the nerve root.
Lumbar spine (L4-L5, L5-S1)
- Acute or chronic low back pain (lumbalgia)
- Pain radiating to the buttock and leg along the sciatic nerve (sciatica)
- Numbness, tingling, "pins and needles" in the foot and toes
- Leg muscle weakness, foot drop
- Pain worsening with coughing, sneezing, straining
- Inability to stand or sit for long periods
- Antalgic posture — forced body position to reduce pain
Cervical spine (C5-C6, C6-C7)
- Neck pain radiating to the shoulder, arm, fingers
- Numbness and tingling in the fingers (often ring finger and little finger)
- Dizziness, tinnitus, visual disturbances
- Occipital headaches
- Arm weakness, impaired fine motor skills
- Limited head rotation and tilting
- With large hernias — impaired coordination, gait
Thoracic spine (Th6-Th12)
- Chest pain, often mimicking angina
- Girdling pain along intercostal nerves
- Numbness in the abdomen or chest area
- Worsening with deep breathing and twisting
- Occurs less frequently, but often with severe neurological symptoms
When to seek urgent care
- Impaired pelvic organ function (urination, defecation)
- Progressive weakness in extremities
- Cauda equina syndrome — emergency condition
- Intractable pain not relieved by analgesics
- Numbness in the perineal area
Diagnosis of Herniated Disc
Accurate diagnosis is the foundation of successful treatment. At MIBRAR® clinic, we use a comprehensive approach combining clinical examination with modern imaging methods.
Diagnostic Methods:
- MRI (magnetic resonance imaging) — the "gold standard" for diagnosing disc herniations. It visualizes soft tissues: disc, nerve roots, spinal cord, ligaments. MRI shows herniation size (accurate to tenths of a millimeter), degree of nerve compression, and condition of adjacent discs
- CT (computed tomography) — complements MRI, especially for assessing bone structures and calcifications
- X-ray — assessment of spinal alignment, disc height, detection of osteophytes and instability
- Electroneuromyography (ENMG) — when necessary, to assess nerve conduction and degree of damage
How MIBRAR® Uses Diagnostics:
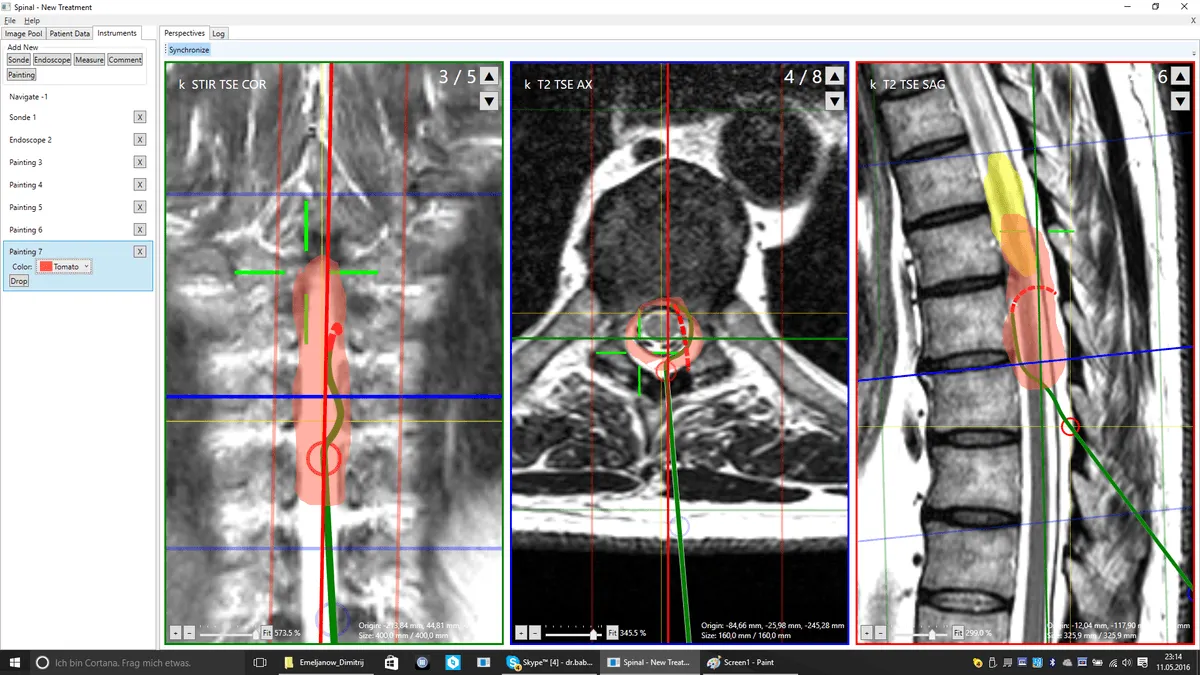
MRI/CT images are uploaded to the Cyber Navi Hand™ navigation system, which creates a 3D model of the patient's spine. On this model, the surgeon plans precise coordinates for micro-invasive access to each damaged disc: insertion angle (accurate to 1°), penetration depth (to 1 mm), and optimal trajectory excluding damage to neural structures.
Free MRI Evaluation
- Send MRI images online
- Prof. Babayan will personally assess your case
- You will receive a report within 48 hours
- No obligations and free of charge
Traditional Treatment vs MIBRAR®
| Criterion | Open Surgery | Epidural Injections | MIBRAR® RRWS |
|---|---|---|---|
| Principle | Surgical removal of herniation | Steroids to reduce inflammation | Disc regeneration using patient's own cells |
| Anesthesia | General anesthesia | Local anesthesia | No general anesthesia (local anesthesia) |
| Incision | 3-6 cm | None | None (puncture 0.3-1.5 mm) |
| Hospitalization | 3-7 days | None | None — home the same day |
| Recovery | 6-12 weeks | 1-3 days | Several days |
| Effect Duration | Variable, recurrences up to 25% | 1-6 months | 10-20+ years (regeneration) |
| Disc Regeneration | ❌ No — disc is removed | ❌ No — pain relief only | ✅ Yes — structural restoration |
| Risks | Recurrence, scarring, infection, instability | Temporary effect, infection risk | Minimal — uses patient's own cells |
How MIBRAR® Treats Herniated Disc
MIBRAR® (Micro-Invasive Biological Regenerative Autologous Reconstruction) is a fundamentally new approach: instead of removing the damaged disc, we initiate its regeneration using the patient's own cells. The procedure is outpatient, without incisions or general anesthesia.
Diagnosis and 3D Planning
MRI/CT scans are uploaded into the navigation system Cyber Navi Hand™ — a development by Prof. Babayan. The program constructs a three-dimensional model of the patient's spine, analyzes anatomical features, and calculates the optimal access trajectory to each damaged disc: insertion angle with accuracy to 1°, penetration depth to 1 mm. This prevents damage to nerve roots and the spinal cord.
Obtaining Regenerative Concentrates
From the patient's venous blood (40-60 ml), CGF (Concentrated Growth Factors) concentrate is obtained — a fibrin matrix saturated with growth factors (PDGF, TGF-β, VEGF, IGF), cytokines, and CD34+ stem cells. The concentration of growth factors in CGF is 5-10 times higher than in regular PRP.
If necessary, from subcutaneous adipose tissue (20-40 ml, lipoaspiration procedure under local anesthesia), Lipogems® concentrate is obtained. Adipose tissue contains 1000 times more mesenchymal stem cells than bone marrow. These cells are capable of differentiating into cartilage tissue cells and initiating regeneration of the damaged annulus fibrosus.
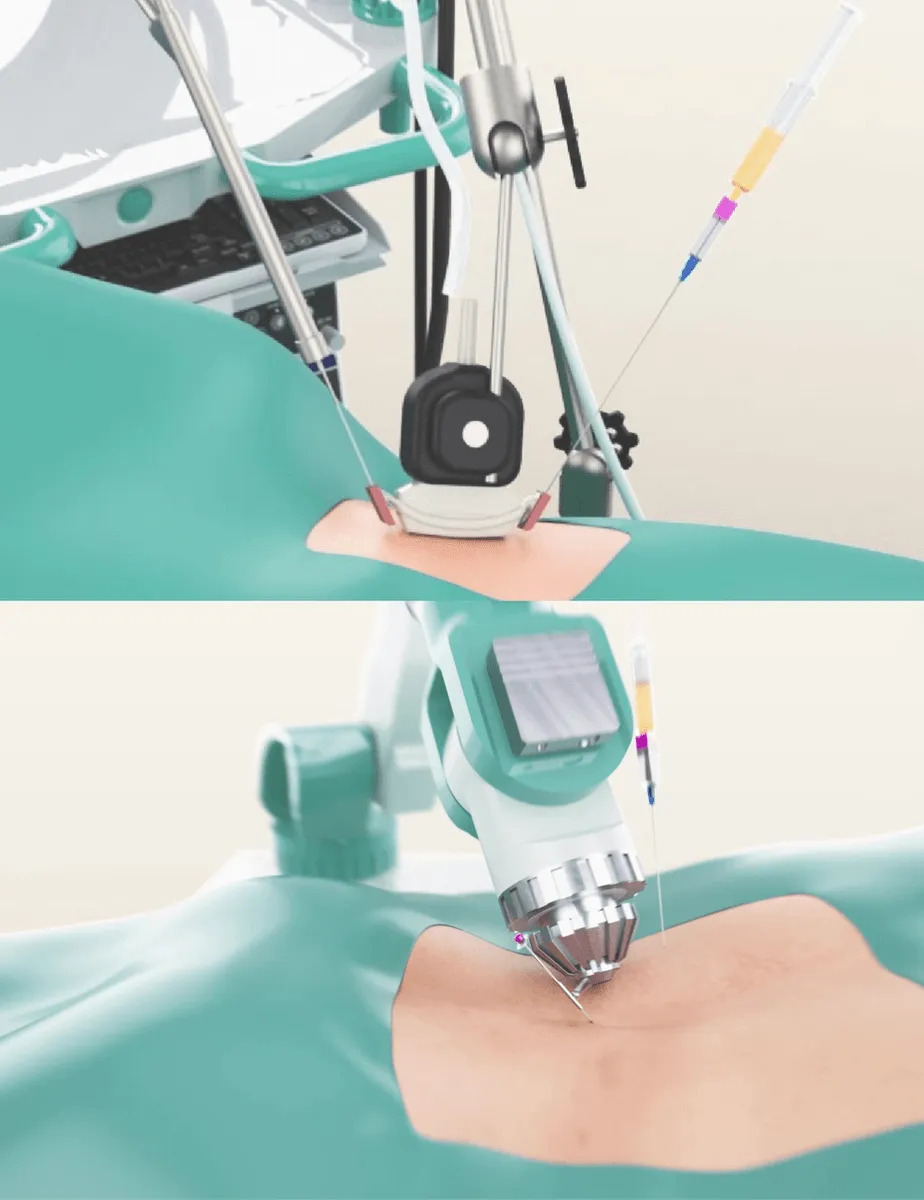
Micro-Invasive Injection
Under C-arm control (fluoroscopic equipment) and Cyber Navi Hand™ navigation, through a puncture sized 0.3-1.5 mm (comparable to an injection needle prick), concentrates are injected directly into the damaged disc and surrounding tissues. Micro-dimensional endoscopes and precision needles of our own design are used. Tissue integrity is restored within a few hours.
Regeneration and Follow-Up
Stem cells and growth factors initiate a cascade of biological processes: regeneration of the annulus fibrosus, restoration of disc hydration and height, reduction of inflammation and edema, restoration of blood supply to surrounding tissues. Regenerative concentrates also have pronounced analgesic and anti-inflammatory properties — most patients report pain reduction within the first days.
Follow-up MRI at 8-16 weeks confirms restoration of disc structure. The regeneration process continues up to 6 months.

Why MIBRAR® Works
The MIBRAR® method is based on a fundamental principle: the human body is capable of regeneration, but to achieve this, "building materials" must be delivered precisely to the site of damage. Studies have shown that stem cells and growth factors, when introduced into the body, primarily migrate to where they are needed most — damaged tissues.
Two Components of Regeneration:
- CGF (Concentrated Growth Factors) — concentrate from the patient's own blood. Contains a fibrin matrix, growth factors (PDGF, TGF-β, VEGF, IGF-1), cytokines, and CD34+ stem cells. The fibrin matrix serves as a "scaffold" for new cells, while growth factors transmit signals to initiate regeneration
- Lipogems® — concentrate of mesenchymal stem cells from adipose tissue. Patented in 2010, clinically available since 2013, used in more than 15,000 patients. In 2016, it was included in the list of 11 best sports medicine technologies in the world (Sports Medicine Technology Awards). Mesenchymal stem cells are capable of differentiating into cartilage, bone, muscle, and ligament cells
Mechanism of Action for Disc Herniation:
- Micro-invasive injection of concentrates directly into the damaged disc
- Stem cells "mark" the damage zone, attracting the body's own regenerative resources
- Growth factors initiate a cascade: chondrocyte proliferation → synthesis of type II collagen → restoration of the annulus fibrosus
- Simultaneously, an anti-inflammatory effect occurs — reduction of edema and compression of nerve roots
- Restoration of nucleus pulposus hydration → restoration of disc height and its shock-absorbing function
Key Difference from All Other Methods: MIBRAR® does not mask pain or remove damaged tissue. The method restores disc structure at the cellular level, which is confirmed by follow-up MRI scans 8-16 weeks after the procedure.
MIBRAR® in Numbers
- 25,000+ procedures performed
- 95% patient satisfaction
- Since 2013 clinical experience
- 0.3-1.5 mm puncture size
- 90 min — 4 hours procedure duration
- 0 days hospitalization
- 8-16 weeks until visible regeneration on MRI
- 10-20+ years duration of effect
Treatment Results for Herniated Disc
Follow-up MRI images clearly show regeneration of damaged discs after the MIBRAR® procedure. Below are real cases from Prof. Babayan's clinic.
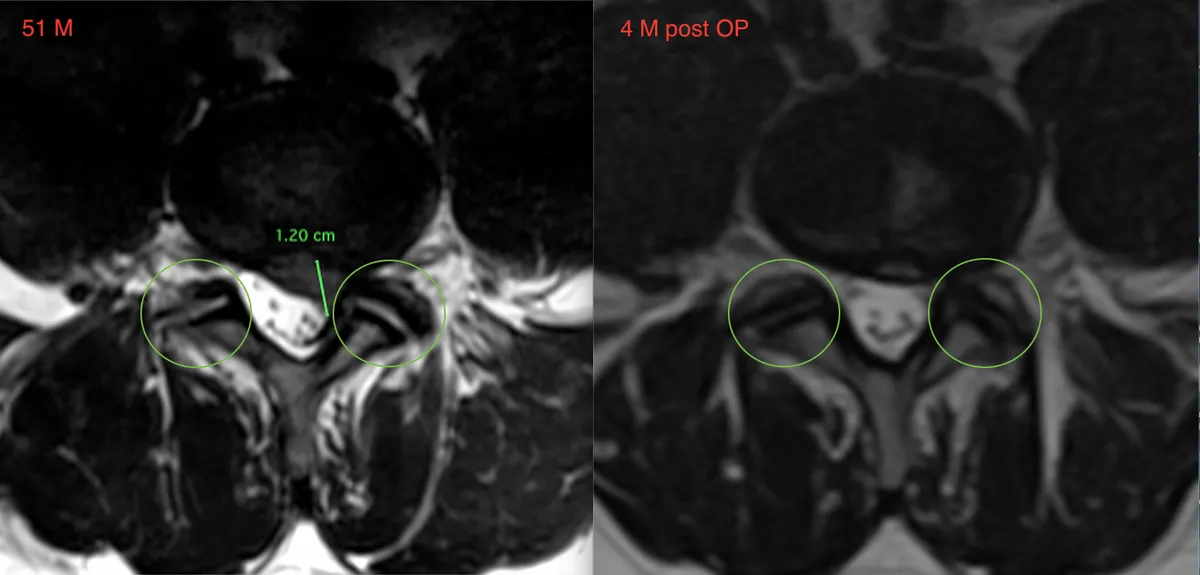
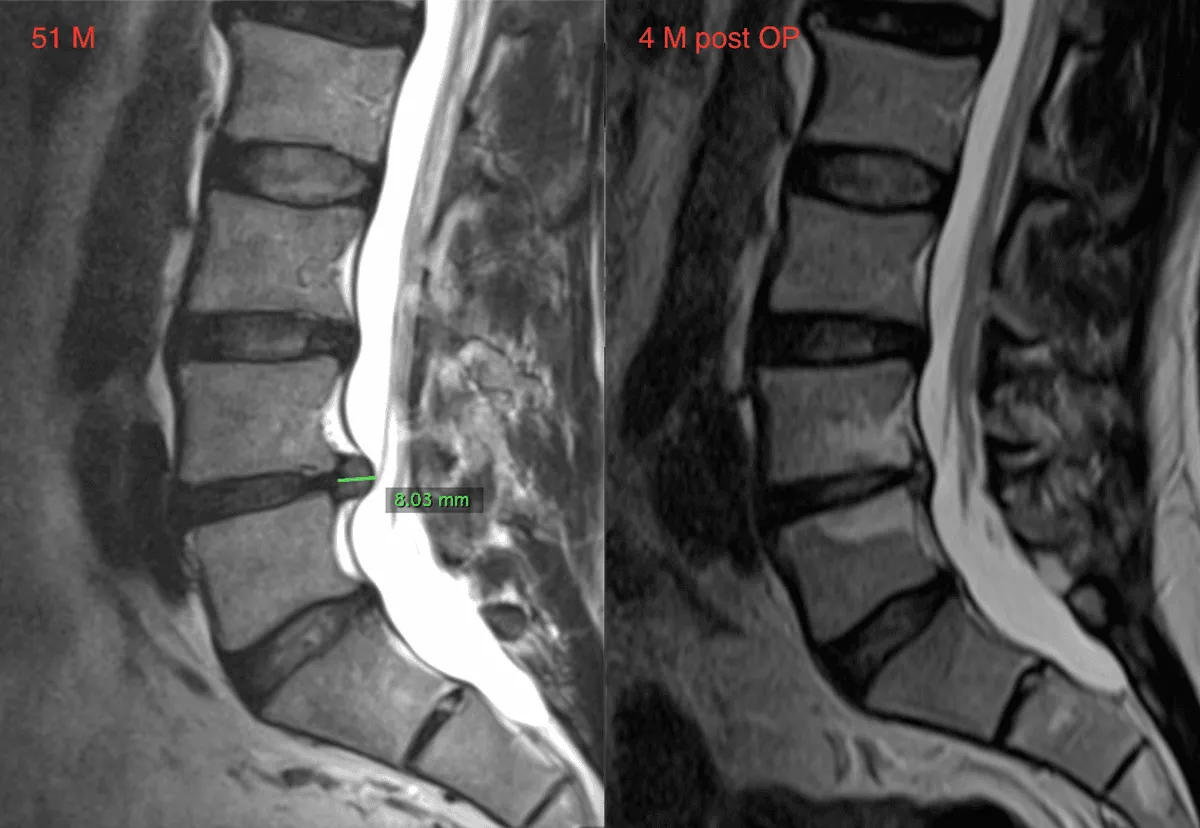
Patient: male, 51 years old
Diagnosis: lumbar disc herniation L5-S1 measuring 1.20 cm (axial view) and 8.03 mm (sagittal view). Significant compression of nerve roots. Sciatica, left leg pain.
Result after 4 months: significant reduction of herniation, restoration of spinal canal patency, complete resolution of nerve root compression. Patient returned to normal activity.
View all treatment results →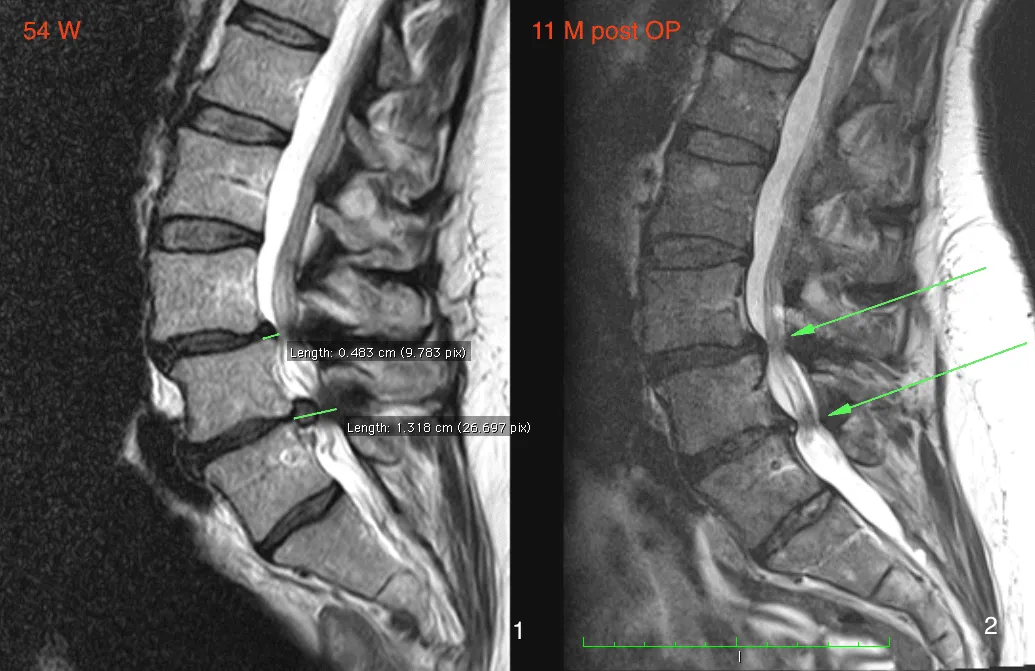
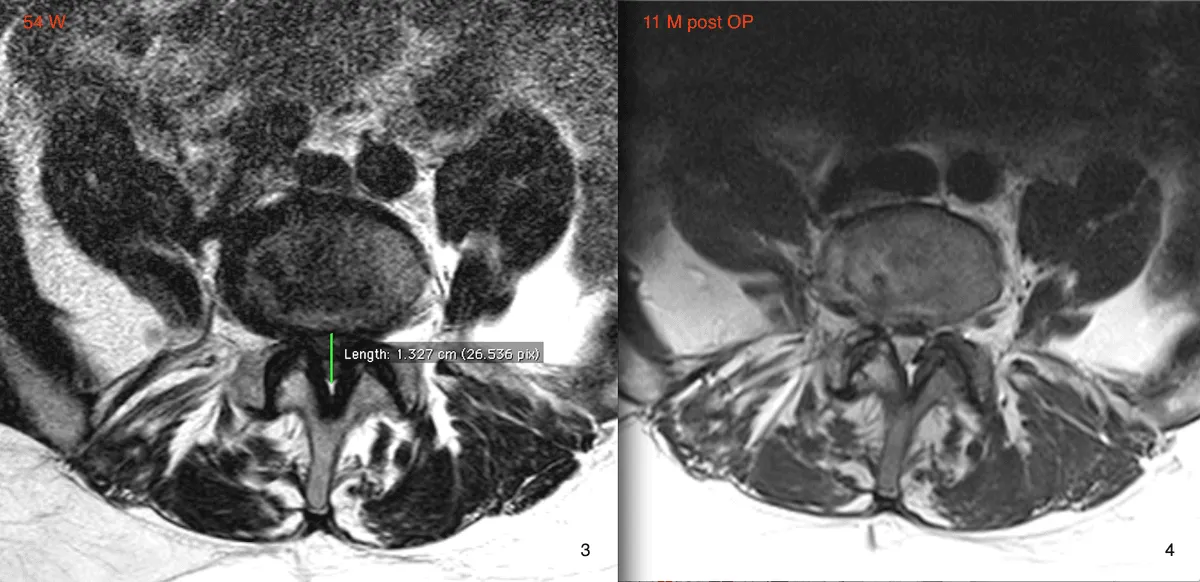
Patient: female, 54 years old
Diagnosis: multiple lumbar disc herniations — 0.483 cm (L4-L5) and 1.316 cm (L5-S1). Chronic pain syndrome for more than 3 years. Conservative treatment without effect. Surgery was recommended but declined by patient.
Result after 11 months: follow-up MRI shows significant regeneration of both discs, restoration of disc space height, substantial reduction of nerve root compression. Pain syndrome completely resolved.
View all treatment results →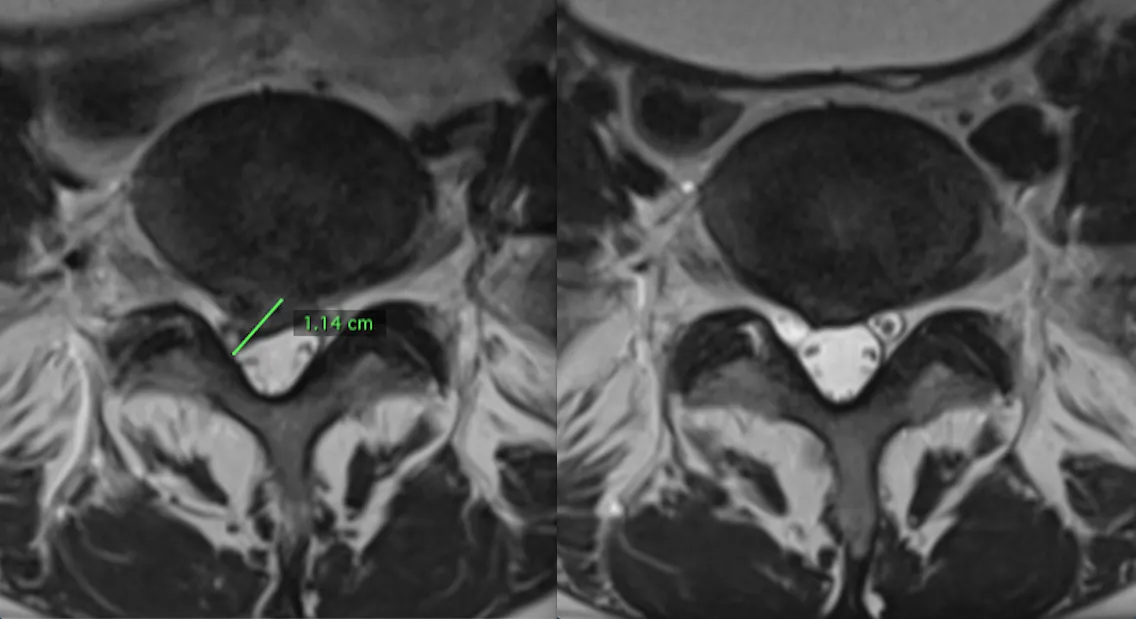
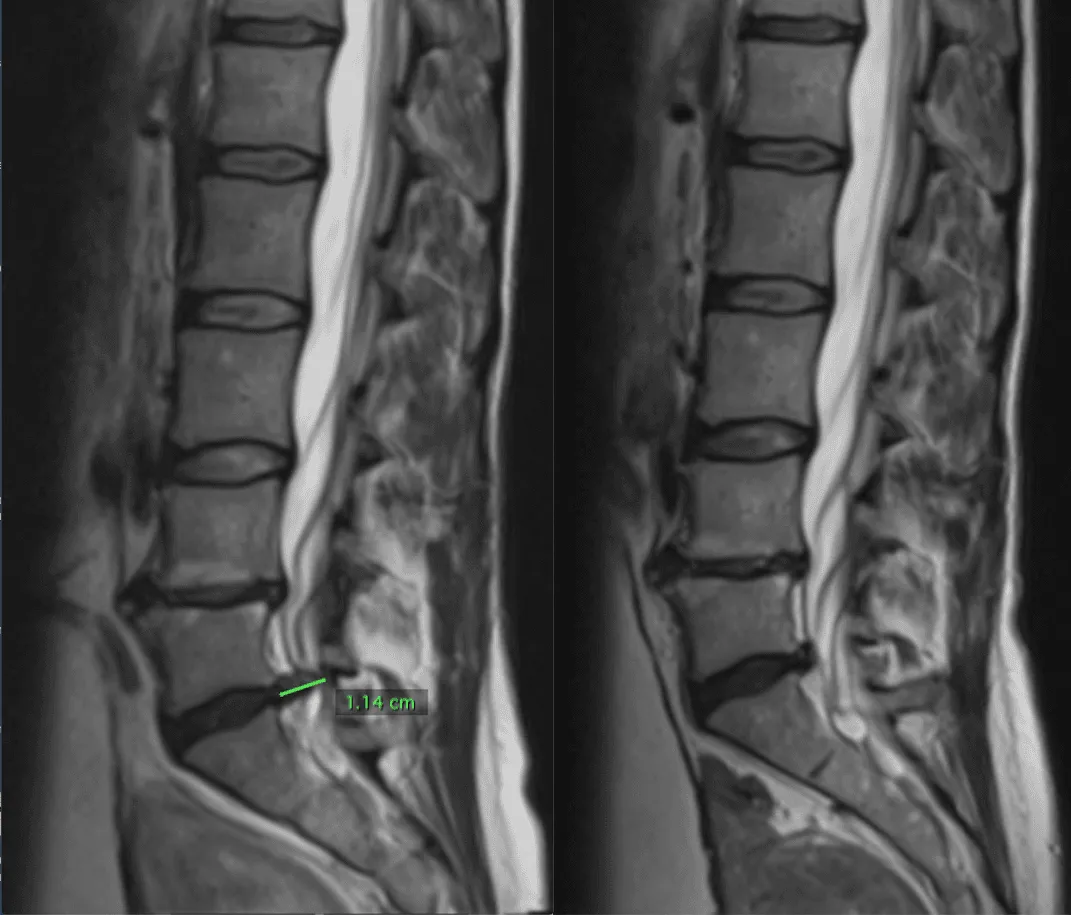
Lumbar Disc Herniation 1.14 cm
Diagnosis: large lumbar disc herniation measuring 1.14 cm with significant compression of the dural sac and nerve roots. On sagittal view (left) — herniation is clearly visible within the spinal canal.
Result: follow-up MRI (right) shows significant regression of herniation, restoration of normal spinal canal anatomy, patent space for neural structures. Axial view confirms reduction of compression.
View all treatment results →MIBRAR® Method Advantages
95% of interventions covered
MIBRAR® covers up to 95% of all spinal neurosurgery and orthopedic operations.
No anesthesia or incisions
Outpatient treatment via 0.3-1.5 mm puncture. No general anesthesia or hospitalization.
No age restrictions
Regeneration at any age. Safe for chronic conditions and anesthesia intolerance.
Rapid improvement
Concentrates have analgesic and anti-inflammatory properties. Relief within days.
Multiple zones at once
Simultaneous treatment of multiple discs or joints in one procedure.
Home the same day
No crutches, braces or rehabilitation needed. MRI follow-up at 8-16 weeks.
MIBRAR® Technology
Cyber Navi Hand™
Intraoperative robotic navigation system. Provides precise access to deep structures with 1 mm and 1 degree accuracy.

Sono Control Arm™
Device for intervention under sonographic control. Eliminates open surgeries with real-time visual monitoring.