
Video about the MIBRAR® Method
What is patellar tendinopathy
"Jumper's knee" — degenerative damage to the patellar ligament (patellar tendon) at its attachment to the inferior pole of the patella. Occurs due to overload of the knee extensor mechanism: jumping, running, weighted squats. One of the main reasons for ending a sports career.
Who is at risk
Jumping sports
Volleyball (up to 45% of players!), basketball (32%), track and field (jumping), handball. Frequency directly correlates with the number of jumps in training.
Running and CrossFit
Running on hard surfaces, CrossFit with box-jumps, weighted squats. Load on the ligament during squatting can reach 8 times body weight.
Strength sports
Weightlifting, powerlifting. Deep squats with heavy weight — maximum load on the patellar ligament.
Blazina stages
Stage 1: Pain only after loading
Discomfort after training, resolves in a few hours. Athlete can train at full volume. Ultrasound shows minimal changes.
Stage 2: Pain at the beginning and after loading
Pain at the start of training, decreases after warm-up, returns afterward. Decreased sports performance. Ultrasound shows thickening, hypoechoic zones.
Stage 3: Constant pain
Pain with daily activities: stairs, standing from a chair, squatting. Inability to participate in sports. Ultrasound shows neovascularization, partial tears.
Stage 4: Complete rupture
Rupture of the patellar ligament. Inability to extend the knee. Requires surgical reconstruction.
Diagnosis
Ultrasound (first line)
Thickening of the proximal portion of the ligament (normal 3-5 mm, in tendinopathy 7-12 mm). Hypoechoic zones of degeneration. Doppler — neovascularization (marker of active process). Dynamic examination with knee flexion.
MRI
Hyperintense signal on T2 in the proximal third of the ligament. Thickening. Detects partial tears, paratendinitis, infrapatellar bursitis. MRI mandatory for Blazina 3-4.
Clinical examination
Tenderness on palpation of the inferior pole of the patella (pathognomonic sign). Pain on single-leg squat (single-leg decline squat test). Victorian Institute of Sport Assessment (VISA-P) — standardized questionnaire.
Treatment Using the MIBRAR® Method
MIBRAR® regenerates damaged tendon tissue — the only method providing structural restoration.
1. Damage Mapping
High-frequency ultrasound with Doppler identifies the precise zone of degeneration and neovascularization for targeted injection.
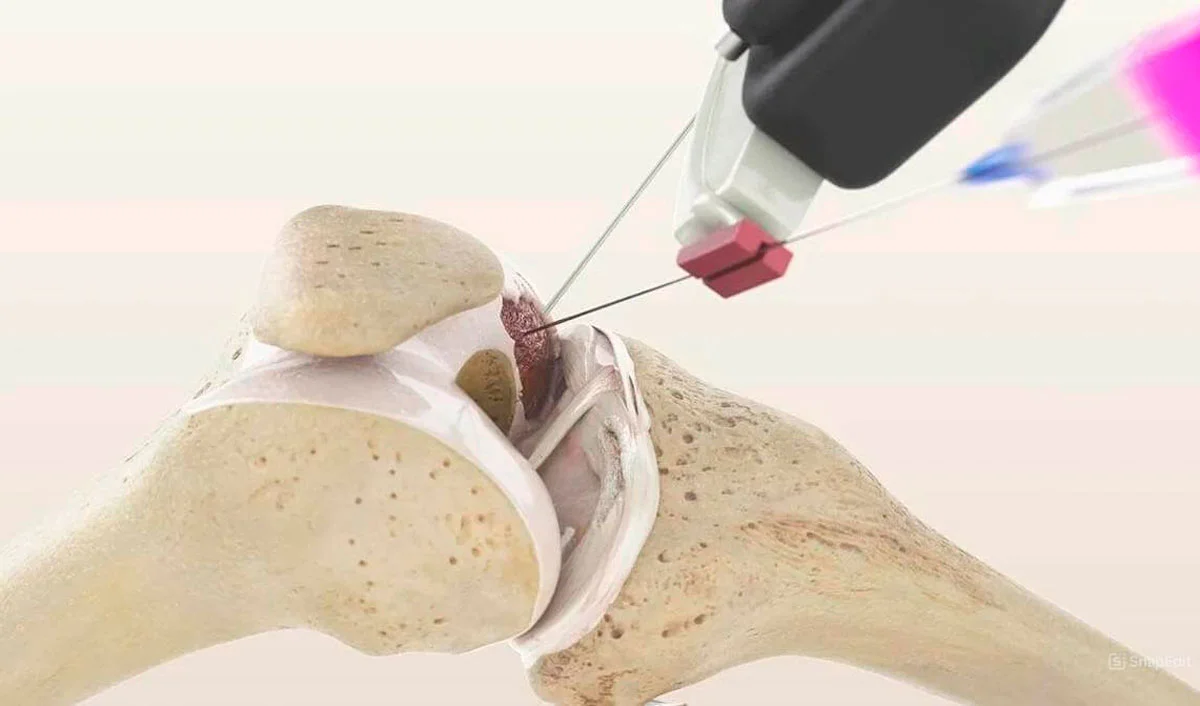
2. CGF + Lipogems® Injection
Under ultrasound guidance, biomaterial is injected in a fan-shaped pattern into the degeneration zone: CGF (growth factors + fibrin scaffold) + Lipogems® (stem cells + extracellular matrix) in severe cases.
3. Regeneration
Stem cells differentiate into tenocytes. TGF-beta, PDGF stimulate type I collagen synthesis. The CGF fibrin scaffold serves as a scaffold for organized tissue growth. Follow-up ultrasound at 3-6 months shows normalization of echostructure and ligament thickness.
Return to Sports
Tendinopathy is not a career-ending diagnosis. MIBRAR® restores the ligament at the cellular level.
Book a ConsultationQuestions about patellar tendinopathy
At stages 1-2 per Blazina — modified loading (remove jumps, deep squats). Eccentric exercises (decline squat) — proven effectiveness. At stage 3 — sports rest until treatment.
Cortisone destroys tendon collagen and increases the risk of complete rupture. This is an absolute contraindication for patellar tendinopathy. Even a single injection is dangerous.
Light activity — after 2 weeks. Running — after 4 weeks. Jumps and sports — after 6-8 weeks. Full collagen reorganization — 3-6 months.
PRP has limited effectiveness (60-70%). MIBRAR® (CGF + Lipogems®) significantly outperforms PRP: CGF contains 10x more growth factors, and Lipogems® stem cells provide true regeneration.